Dental Students Compare Conventional and 3D Printed Surgical Training Models


There are few things I hate more than going to the dentist. That’s why I’m always glad to hear stories of dental students using 3D printed training models to learn on – if they have to work in my mouth, then I want them to know what they’re doing. A group of researchers from University Hospital Münster in Germany published a paper on this topic, relaying the results of their work using real patient data to create 3D printed surgical training models for root tip resection. Then, they compared them against a commercial typodont model, which is a common simulation model used at university dental clinics with replaceable gingiva masks and teeth that often “show idealized eugnathic situations, which are rarely encountered in everyday practice.”
“Furthermore, the ready-made standard models do not usually depict special pathological or anatomic situations,” they wrote.
A root tip resection, or apicoectomy, removes inflammation around the tip of the tooth’s root. The researchers explained that the typodont model at their university features teeth “in direct contact with the hard plastic that simulates the jawbone,” and simulates the inflammation (apical granuloma) with wax, though it’s missing a sensitive periodontal ligament.
“The teeth used are idealized stereotypes. Anatomical variations, such as extremely long or even curved roots, cannot be simulated with these industrially produced models. Therefore, we have developed a method to create more realistic, individualized training models,” the researchers explain.
The model they created is of a real patient’s upper jaw with three anterior root apices, periodontal ligament, and the apical granuloma, along with a gingival mask.
“We also present an evaluation of the model by dental students and compare it with their evaluation of the conventional typodont model,” the team wrote. “Our intention was to evaluate whether dental students accept the 3D-printed surgical training model just as well as the popular typodont model.”

L-R: Modified plaster cast, modified plaster cast with wax layer.
They used CAD/CAM technology to design the training model, which allowed them to add the simulated inflamed tissue, and took a conventional impression of the area in question in order to make a plaster cast. The gingiva was modeled with a 1 mm thick layer of wax, and an industrial 3D scanner was used to attain the shape of the modified cast with and without the wax gingival mask.

L-R: Scanned surface of the plaster cast without wax layer and meshes of the three teeth aligned to the upper jaw.
The cone beam computed tomography (CBCT) data of another patient was used to create 3D models/meshes of teeth 11, 12, and 21 in Materialise Mimics, and the 3D reconstruction was modified using Rhinoceros 5. To make a model of the periodontal ligament, which the typodont model doesn’t include, they deleted the upper parts of the teeth mesh and thickened the rest by 0.25 mm in Geomagic Wrap.
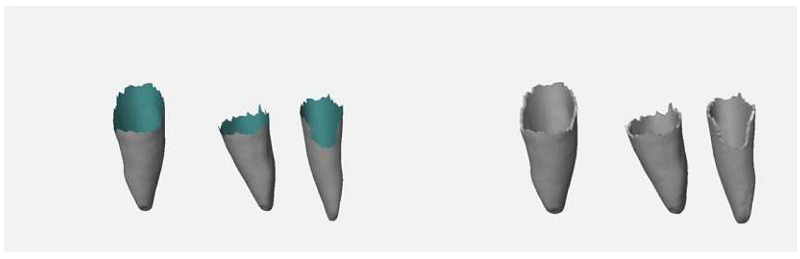
L-R: Meshes of the roots (rear faces of mesh in blue-green), extruded root surfaces representing periodontal ligament.
They constructed a 6 mm sphere around the root apex of tooth 11 to simulate an apical granuloma.
“The material used to represent the periodontal ligament and the apical granuloma is softer than the material used for the other parts of the model. This allows a more realistic representation than in the typodont model,” they explained.

Meshes of the granuloma on tooth 11 and the periodontal ligament on teeth 11, 12 and 21, 3D printed in soft support material (red).
The 3D printed model also includes a silicone gingival mask so students can practice the surgical incision. A 3D printed matrix technique was used to fabricate the mask directly onto the model, and the model was 3D printed out of liquid photopolymer on an Objet Eden 260V PolyJet 3D printer. The undercut areas and the cavities in the model that simulated apical granuloma and periodontal ligament were filled with a soft support material. It took roughly six hours to 3D print 12 models in a single build.

Silicone gingival mask.
“Dental students, about one year before their final examinations, acted as test persons and evaluated the simulation models on a visual analogue scale (VAS) with four questions (Q1–Q4),” the researchers wrote.
35 students evaluated the typodont model, while 33 students used the 3D printed simulation model. Participants watched a video of the root tip resection exercise, and then completed the procedure once. They were given a questionnaire about the simulation model and the difficulty of the exercise, rated on a visual analogue scale (VAS). There was also an optional free-text section if a participant wanted to express their opinion in their own words.
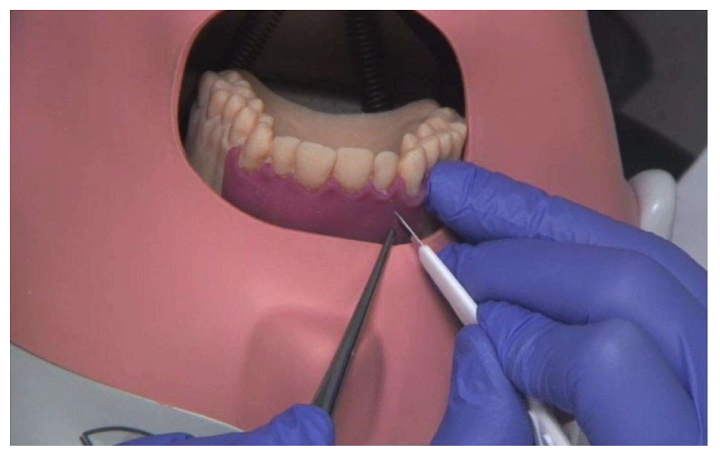
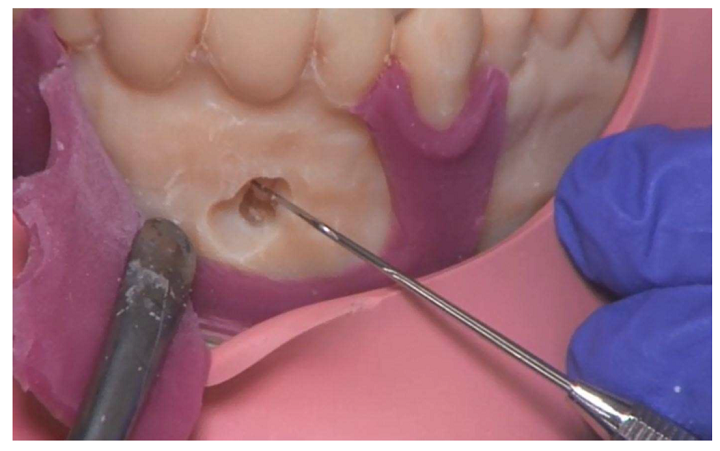
Surgical incision guidance on the 3D printed model in the phantom.

Osteotomy of the root tip.

Presentation of the root tip. Note: torn gingiva mask.
Resected root tip with demarcation to the bone.
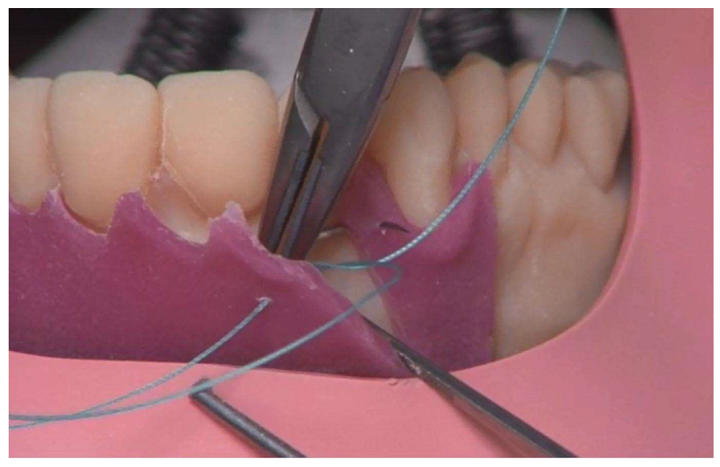
Suture exercise on the gingiva mask.
54.5% of the Group 2 participants said in the free-text section that the gingiva mask in the 3D printed model tore during the procedure, while 20% in Group 1 said that it detached from the typodont model.
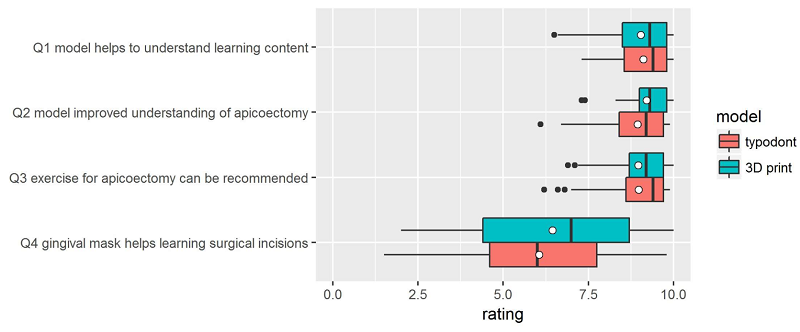
Questionnaire results; white dots denote the mean values.
“Shapiro–Wilk normality tests revealed that, with the exception of Q4, normality cannot be assumed,” they explained. “Wilcoxon rank sum tests were therefore carried out to identify differences in the assessments of the two model types. The alternative hypothesis for each test was “The rating for the typodont model is higher than that for the 3D printed”. As the p-values presented in Table 1 reveal, the alternative hypothesis has to be rejected in all cases.”

Table 1.
The researchers determined that their 3D printed training models were “not inferior to the industrially manufactured typodont models,” and that the approach is very flexible – the models can be easily redesigned and adapted for different learning scenarios, and it’s much faster to fix them when necessary. While the 3D printers weren’t cheap, the material costs for a 3D printed single-use model were only about €10, compared to €300 for the multi-use hypodont model.
“A shortcoming of our study is that the exercises were performed by students without surgical experience. As a result, there is a lack of professional evaluation of the models in terms of how well they reflect the reality. Thus, we were not able to check an important quality aspect of the models,” the researchers noted.
“Future studies with experienced surgeons could provide more information about the realism of the 3D-printed models.”
Other issues include the missing color difference between anatomical structures or cortical and cancellous bone structures, and the gingiva mask needs improvement, either through alternative technologies or materials.
“Individual 3D-printed surgical training models based on real patient data offer a realistic alternative to industrially manufactured typodont models. However, there is still room for improvement with respect to the gingiva mask for learning surgical incision and flap formation,” they concluded.
Discuss this and other 3D printing topics at 3DPrintBoard.com or share your thoughts below.
Subscribe to Our Email Newsletter
Stay up-to-date on all the latest news from the 3D printing industry and receive information and offers from third party vendors.
Print Services
Upload your 3D Models and get them printed quickly and efficiently.










You May Also Like
Beehive Industries Invests $70M in Ohio to Support Its Advanced Manufacturing Buildup for Propulsion
Beehive Industries and the state of Ohio have each been killing it in the metal 3D printing game. Naturally then, it was only logical for Beehive and Ohio to combine...
3D Printing News Briefs, June 10, 2026: Grand Opening, Photoresins, Footwear, & More
We’re starting with some exciting news in today’s 3D Printing News Briefs: Stratasys just celebrated the opening of its new North American headquarters in Minnesota. Moving on, Nanoscribe is scaling...
Chromatic 3D Materials To Make Rocket Propellant
Chromatic 3D Materials makes cost-effective, tough elastomeric materials. Its process is being used to make industrial parts at scale. Now the film has turned into rocket propellant. The firm is...
Fleet Readiness Centers, a Six-Month Metal AM Push, and Shifting Defense Procurement
As I wrote about earlier this month, the Trump administration has requested a record $1.5 trillion in Department of Defense (DoD) funding for FY 2027. In my post about what...