Complete Tumor 3D Printed to Facilitate Faster Treatment Prediction

There are more than 120 different types of brain tumors, many of which are cancerous, but the deadliest, and sadly most common, is the aggressive, fast-growing glioblastoma multiforme (GBM), a type of central nervous system tumor that forms on the brain’s supportive tissue. For several years now, researchers have been turning to 3D technologies to help better understand and treat this lethal disease, and the latest efforts are by a team of Tel Aviv University researchers, who used 3D bioprinting to fabricate an entire active, viable glioblastoma tumor.
The tumor, printed out of human glioblastoma tissues taken from actual patients at the Tel Aviv Sourasky Medical Center, includes a system of tubes, akin to blood vessels, that allow drugs and blood cells alike to flow through, in a simulation of an actual tumor. Led by Professor Ronit Ronit Satchi-Fainaro, Sackler Faculty of Medicine and Sagol School of Neuroscience, and PhD student Lena Neufeld, the results of the study were recently published in Science Advances.
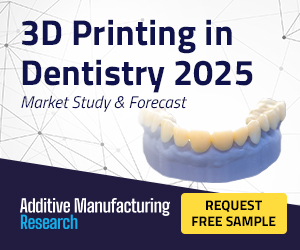
 Bio-mechanical characterization determined the bioink composition that best mimics the elasticity and composition of the brain tissue. (A) G′ of fibrin 3D-bioink formation at different Th concentrations with 3% (w/v) TG at 37°C (average shown of n= 3 per group). (B) Young’s modulus of fibrin 3D-bioink at different concentrations of gelatin [3%, 6%, and 12% (w/v)] with 3% (w/v) TG and Th (0. 5 U/ml) as a clear bioink and as a cell-laden bioink composed of PD-GB4 or GL261 at 1 × 106cells/ml (n = 8 to 13 per group). (C) Swelling at equilibrium of fibrin 3D-bioink at different concentrations of gelatin [3%, 6%, and 12% (w/v)] with 3% (w/v) TG and Th (0.5 U/ml) (n = 8 per group). (D) Growth curves at different concentrations of gelatin [3%, 6%, and 12% (w/v)] with 3% (w/v) TG and 0. 5 U/ml of Th of GL261 [top: 3% (w/v) versus 6% (w/v), P < 0.00001; 6% (w/v) versus 12% (w/v), P < 0.00001; 3% (w/v) versus 12% (w/v), P = 0.002 by t test] and PD-GB4 [bottom: 3% (w/v) versus 6% (w/v), P = 0.0004; 6% (w/v) versus 12% (w/v), P = 0.0004, by t test] in fibrin 3D-bioink (n = 4 per group). (E) Representative images demonstrating the morphology of mCherry-labeled GL261 (top) and iRFP-labeled PD-GB4 cells (bottom) following 14 days in fibrin 3D-bioink [6% (w/v) gelatin, 3% (w/v) TG, and Th (0.5 U/ml)]. Cells were analyzed by live confocal Z-stack imaging of the whole bioink and by fluorescence imaging and H&E staining of bioink sections (n = 3 to 4 per group). Scale bars, 100 μm.
Bio-mechanical characterization determined the bioink composition that best mimics the elasticity and composition of the brain tissue. (A) G′ of fibrin 3D-bioink formation at different Th concentrations with 3% (w/v) TG at 37°C (average shown of n= 3 per group). (B) Young’s modulus of fibrin 3D-bioink at different concentrations of gelatin [3%, 6%, and 12% (w/v)] with 3% (w/v) TG and Th (0. 5 U/ml) as a clear bioink and as a cell-laden bioink composed of PD-GB4 or GL261 at 1 × 106cells/ml (n = 8 to 13 per group). (C) Swelling at equilibrium of fibrin 3D-bioink at different concentrations of gelatin [3%, 6%, and 12% (w/v)] with 3% (w/v) TG and Th (0.5 U/ml) (n = 8 per group). (D) Growth curves at different concentrations of gelatin [3%, 6%, and 12% (w/v)] with 3% (w/v) TG and 0. 5 U/ml of Th of GL261 [top: 3% (w/v) versus 6% (w/v), P < 0.00001; 6% (w/v) versus 12% (w/v), P < 0.00001; 3% (w/v) versus 12% (w/v), P = 0.002 by t test] and PD-GB4 [bottom: 3% (w/v) versus 6% (w/v), P = 0.0004; 6% (w/v) versus 12% (w/v), P = 0.0004, by t test] in fibrin 3D-bioink (n = 4 per group). (E) Representative images demonstrating the morphology of mCherry-labeled GL261 (top) and iRFP-labeled PD-GB4 cells (bottom) following 14 days in fibrin 3D-bioink [6% (w/v) gelatin, 3% (w/v) TG, and Th (0.5 U/ml)]. Cells were analyzed by live confocal Z-stack imaging of the whole bioink and by fluorescence imaging and H&E staining of bioink sections (n = 3 to 4 per group). Scale bars, 100 μm.“Glioblastoma is the most lethal cancer of the central nervous system, accounting for most brain malignancies. In a previous study, we identified a protein called P-Selectin, produced when glioblastoma cancer cells encounter microglia — cells of the brain’s immune system. We found that this protein is responsible for a failure in the microglia, causing them to support rather than attack the deadly cancer cells, helping the cancer spread,” explained Prof. Satchi-Fainaro, who is also the Director of the Cancer Biology Research Center, Head of the Cancer Research and Nanomedicine Laboratory, and Director of the Morris Kahn 3D-BioPrinting for Cancer Research Initiative, all at the university. “However, we identified the protein in tumors removed during surgery, but not in glioblastoma cells grown on 2D plastic petri dishes in our lab. The reason is that cancer, like all tissues, behaves very differently on a plastic surface than it does in the human body. Approximately 90% of all experimental drugs fail at the clinical stage because the success achieved in the lab is not reproduced in patients.”
Eilam Yeini, Noa Reisman, Yael Shtilerman, Dr. Dikla Ben-Shushan, Sabina Pozzi, Dr. Galia Tiram, Dr. Anat Eldar-Boock, and Dr. Shiran Farber—other researchers at Prof. Satchi-Fainaro’s laboratory—helped Neufeld develop this new technology. The bioprinted glioblastoma tumor model includes 3D cancer tissue that’s surrounded by an extracellular matrix, which uses functional blood vessels to communicate with its microenvironment and solve the problem about cancer behaving differently in the human body than it does on plastic.
“It’s not only the cancer cells. It’s also the cells of the microenvironment in the brain; the astrocytes, microglia and blood vessels connected to a microfluidic system — namely a system enabling us to deliver substances like blood cells and drugs to the tumor replica,” Prof. Satchi-Fainaro said. “Each model is printed in a bioreactor we have designed in the lab, using a hydrogel sampled and reproduced from the extracellular matrix taken from the patient, thereby simulating the tissue itself. The physical and mechanical properties of the brain are different from those of other organs, like the skin, breast, or bone. Breast tissue consists mostly of fat, bone tissue is mostly calcium; each tissue has its own properties, which affect the behavior of cancer cells and how they respond to medications. Growing all types of cancer on identical plastic surfaces is not an optimal simulation of the clinical setting.”
 3D brain-mimicking bioink is biocompatible and promotes long-term cell viability of GB cells and brain stromal cells. (A) Representative immunostaining images of GFAP (top, in green) or IBA1 (bottom, in green) in fibrin 3D-bioink seeded with GB and stromal cells cocultured for 7 days. Images depict Hoechst-stained nucleus (in blue), iRFP-labeled PD-GB cells (PD-GB4; in cyan). Scale bars, 100 μm. (B) Growth curves of PD-GB cells (PD-GB4), alone or cocultured with hAstro (1:1 ratio) in fibrin 3D-bioink (P = 0.004, t test; n = 4 per group). (C) The invasion of iRFP-labeled PD-GB4 cells from the inner core to the surrounding area in the absence or presence of hAstro (1 × 106 cells/ml) was evaluated by fluorescent microscopy imaging. The invasion was calculated as the total area density in outer bioink and quantified using ImageJ by RLU (P = 0.004, t test; n = 12 per group). Representative images of cell invasion are shown; dashed lines delineate the edge between the core and the surrounding tissue according to the images on day 1. Scale bars, 100 μm. (D) SEM images of acellular fibrin 3D-bioink (top left); cell-laden fibrin 3D-bioink composed of patient-derived PD-GB4 cells, hAstro, and hMG cells (bottom left); healthy hemisphere of a C57BL/6 mouse (top right); and GL261 tumor-containing hemisphere of the same mouse (bottom right). Scale bars, 10 μm. The pore size diameter of each group was quantified using ImageJ (n = 2 to 20 photos per group, n = 13 to 170 measurements in each photo) and showed that enlarged and diverse pore sizes characterized the cell-laden bioink and brain tissue bearing the GB tumor.
3D brain-mimicking bioink is biocompatible and promotes long-term cell viability of GB cells and brain stromal cells. (A) Representative immunostaining images of GFAP (top, in green) or IBA1 (bottom, in green) in fibrin 3D-bioink seeded with GB and stromal cells cocultured for 7 days. Images depict Hoechst-stained nucleus (in blue), iRFP-labeled PD-GB cells (PD-GB4; in cyan). Scale bars, 100 μm. (B) Growth curves of PD-GB cells (PD-GB4), alone or cocultured with hAstro (1:1 ratio) in fibrin 3D-bioink (P = 0.004, t test; n = 4 per group). (C) The invasion of iRFP-labeled PD-GB4 cells from the inner core to the surrounding area in the absence or presence of hAstro (1 × 106 cells/ml) was evaluated by fluorescent microscopy imaging. The invasion was calculated as the total area density in outer bioink and quantified using ImageJ by RLU (P = 0.004, t test; n = 12 per group). Representative images of cell invasion are shown; dashed lines delineate the edge between the core and the surrounding tissue according to the images on day 1. Scale bars, 100 μm. (D) SEM images of acellular fibrin 3D-bioink (top left); cell-laden fibrin 3D-bioink composed of patient-derived PD-GB4 cells, hAstro, and hMG cells (bottom left); healthy hemisphere of a C57BL/6 mouse (top right); and GL261 tumor-containing hemisphere of the same mouse (bottom right). Scale bars, 10 μm. The pore size diameter of each group was quantified using ImageJ (n = 2 to 20 photos per group, n = 13 to 170 measurements in each photo) and showed that enlarged and diverse pore sizes characterized the cell-laden bioink and brain tissue bearing the GB tumor.The team’s guess was that current cancer models are inadequate because they don’t have the necessary interactions between the tumor and stroma—the supportive tissue of an organ or tumor made up of blood vessels and connective tissues.
“Therefore, we recapitulated the tumor heterogenic microenvironment by creating fibrin glioblastoma bioink consisting of patient-derived glioblastoma cells, astrocytes, and microglia. In addition, perfusable blood vessels were created using a sacrificial bioink coated with brain pericytes and endothelial cells,” the researchers explained in their paper.
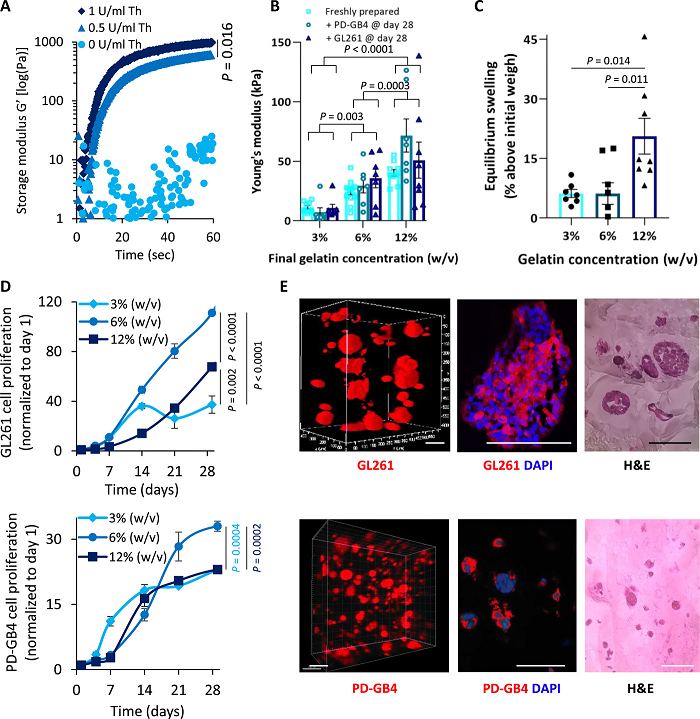
 Fibrin brain-mimicking 3D-bioink integrated with 3D engineered printed perfusable vascular network. (A) Schematic illustration of the 3D-bioprinting model multistage process. (B) 3D-printed Pluronic-based vascular bioink (in cyan) on top of 3D-printed layers of fibrin 3D GB-stroma bioink (in white). (C) 3D-bioprinted vascularized GB model sealed in a metal frame showing the complete perfusion chip. (D) The vascularized 3D-bioprinted GB model is connected to a peristaltic pump through a tubing system, placed in a designated incubator. (E) Tiled Z-stack confocal microscopy images of the 3D-printed penta-culture vascularized GB model. Blood vessels are lined with iRFP-labeled hPericytes (in cyan) together with mCherry-labeled HUVEC (in red) (107 cells/ml; 4:1 ratio) and surrounded by azurite-labeled PD-GB4 (in blue), GFP-labeled hAstro (in green), and nonlabeled hMG (2.1 × 106 cells/ml; 1:1:0.1 ratio). The dashed box represents a coronal cross-sectional plane of the vessel. (F) Fluorescence microscopy images of the 3D-bioprinted vascularized GB model before (top) and after (bottom) perfusion of 70-kDa dextran-FITC. The 3D-bioprinted model is composed of a fluorescently labeled vascular network (mCherry-labeled HUVEC and iRFP-labeled hPericytes) surrounded by nonlabeled GB-bioink (hAstro, PD-GB4, and hMG).
Fibrin brain-mimicking 3D-bioink integrated with 3D engineered printed perfusable vascular network. (A) Schematic illustration of the 3D-bioprinting model multistage process. (B) 3D-printed Pluronic-based vascular bioink (in cyan) on top of 3D-printed layers of fibrin 3D GB-stroma bioink (in white). (C) 3D-bioprinted vascularized GB model sealed in a metal frame showing the complete perfusion chip. (D) The vascularized 3D-bioprinted GB model is connected to a peristaltic pump through a tubing system, placed in a designated incubator. (E) Tiled Z-stack confocal microscopy images of the 3D-printed penta-culture vascularized GB model. Blood vessels are lined with iRFP-labeled hPericytes (in cyan) together with mCherry-labeled HUVEC (in red) (107 cells/ml; 4:1 ratio) and surrounded by azurite-labeled PD-GB4 (in blue), GFP-labeled hAstro (in green), and nonlabeled hMG (2.1 × 106 cells/ml; 1:1:0.1 ratio). The dashed box represents a coronal cross-sectional plane of the vessel. (F) Fluorescence microscopy images of the 3D-bioprinted vascularized GB model before (top) and after (bottom) perfusion of 70-kDa dextran-FITC. The 3D-bioprinted model is composed of a fluorescently labeled vascular network (mCherry-labeled HUVEC and iRFP-labeled hPericytes) surrounded by nonlabeled GB-bioink (hAstro, PD-GB4, and hMG).The team based its 3D engineered tissue constructs on a tumor bioink, made up of the natural polymers gelatin and fibrinogen, and a vascular bioink, composed of thermo-reversible biocompatible synthetic polymer Pluronic F127. As the researchers explained, due to its reversible gelation process, Pluronic F127 served as a sacrifical material “to fabricate embedded vasculature inside the 3D model and liquefied to create a 3D lumen vascular structure.”
They found that the 3D bioprinted model was more effective in terms of rapid, reproducible prediction of cancer treatment than petri dish cancer cells, which grow tumors and spread at the same rate. The researchers first tested a substance with the P-Selectin protein in glioblastoma cell cultures grown in 2D petri dishes, and found that there was no difference in cell division and migration between the control cells and the treated cells. But, by blocking this protein in animal models and their bioprinted model, they could successfully delay growth and invasion of glioblastoma.
 Treatment with SELPi resulted in a substantial reduction in GB cell proliferation in fibrin 3D-bioink compared to 2D culture. (A to C) Response of PD-GB4 (A), T98G-F (B), and U-87MG-F (C) to treatment with SELPi in 2D culture (left, n = 3 per group) and in 3D-bioink (center, n = 8/12 per group), representative images of labeled cells at the end of evaluation. Scale bars, 100 μm. Flow cytometry analysis of P-selectin expression of cells grown in 2D culture and in fibrin 3D-bioink (right, n = 3 per group).
Treatment with SELPi resulted in a substantial reduction in GB cell proliferation in fibrin 3D-bioink compared to 2D culture. (A to C) Response of PD-GB4 (A), T98G-F (B), and U-87MG-F (C) to treatment with SELPi in 2D culture (left, n = 3 per group) and in 3D-bioink (center, n = 8/12 per group), representative images of labeled cells at the end of evaluation. Scale bars, 100 μm. Flow cytometry analysis of P-selectin expression of cells grown in 2D culture and in fibrin 3D-bioink (right, n = 3 per group).“In addition, collaborating with the lab of Dr. Asaf Madi of the Department of Pathology at TAU’s Faculty of Medicine, we conducted genetic sequencing of the cancer cells grown in the 3D-bioprinted model, and compared them to both cancer cells grown on 2D plastic and cancer cells taken from patients. Thus, we demonstrated a much greater resemblance between the 3D-bioprinted tumors and patient-derived glioblastoma cells grown together with brain stromal cells in their natural environment. Through time, the cancer cells grown on plastic changed considerably, finally losing any resemblance to the cancer cells in the patient’s brain tumor sample,” Prof. Satchi-Fainaro said.
The major result of this experiment was proof that many potentially effective cancer drugs often don’t make it to human patients because they fail 2D model tests. The researchers believe that their new approach will enable new drug discovery and faster treatment predictions, and eventually expedite personalized medicine for cancer patients.
 Schematic illustration of the methodological approach using a perfusable microengineered vascular 3D bioprinted tumor model for drug screening and target discovery. MRI, magnetic resonance imaging; μ-CT, micro–computed tomography.
Schematic illustration of the methodological approach using a perfusable microengineered vascular 3D bioprinted tumor model for drug screening and target discovery. MRI, magnetic resonance imaging; μ-CT, micro–computed tomography.“If we take a sample from a patient’s tissue, together with its extracellular matrix, we can 3D-bioprint from this sample 100 tiny tumors and test many different drugs in various combinations to discover the optimal treatment for this specific tumor. Alternately, we can test numerous compounds on a 3D-bioprinted tumor and decide which is most promising for further development and investment as a potential drug,” concluded Prof. Satchi-Fainaro. “But perhaps the most exciting aspect is finding novel druggable target proteins and genes in cancer cells — a very difficult task when the tumor is inside the brain of a human patient or model animal. Our innovation gives us unprecedented access, with no time limits, to 3D tumors mimicking better the clinical scenario, enabling optimal investigation.”
(Source: ScienceDaily)
Subscribe to Our Email Newsletter
Stay up-to-date on all the latest news from the 3D printing industry and receive information and offers from third party vendors.
Print Services
Upload your 3D Models and get them printed quickly and efficiently.









You May Also Like
3D Printing Financials: Materialise Stays Profitable in Q2 Thanks to Medical Division
The second quarter of 2025 was a balancing act for Materialise (Nasdaq: MTLS), with strong momentum in its medical segment and slower performance across other parts of the business. Like...
Protolabs Installs Second Axtra3D Lumia X1 to Meet Growing Demand for Photopolymers
Digital manufacturing leader Protolabs offers many services, including injection molding, CNC machining, and 3D printing, which makes it versatile enough to serve a wide range of customer needs. While the...
Printing Money Episode 30: Q1 2025 Public 3D Printing Earnings Review with Troy Jensen, Cantor Fitzgerald
Printing Money is back with Episode 30, and it’s that quarterly time, so we are happy and thankful to welcome back Troy Jensen (Managing Director, Cantor Fitzgerald) to review the...
Protolabs Brings in New CEO, Keeps Growth Plans on Track
A new CEO is stepping in at Protolabs (NYSE: PRLB). This week, the digital manufacturing company announced that Suresh Krishna is now its President and CEO. Krishna is stepping into...