Justin Ryan of Rady Children’s Hospital on 3D Printing in Hospitals


I’ve rarely seen a trend go so glacially slow and then speed up so rapidly as 3D printing labs in US hospitals. For years there were only one or two pioneers such as Albert Woo trying to establish 3D printing labs in hospitals. Using 3D printing for phantoms, education and surgical planning was a niche activity. If hospitals did use surgical models either to help complex procedures or to help educate patients or staff they usually outsourced the work. Now in a few short years, it seems like every major US hospital has an internal 3D printing lab. There are over a 150 at last count and the number is growing every day. Now with hospitals being able to seek reimbursement the trend should only accelerate. To me it will be fascinating to see how hospitals will continue to use 3D printing and how uses will evolve. Will internal 3D printing capacity mean that hospitals will produce their own braces or surgical guides or will they stick strickly to demo models? Will all the cool applications get stuck in Legal or will this lead to changes in beds and operating theaters globally?
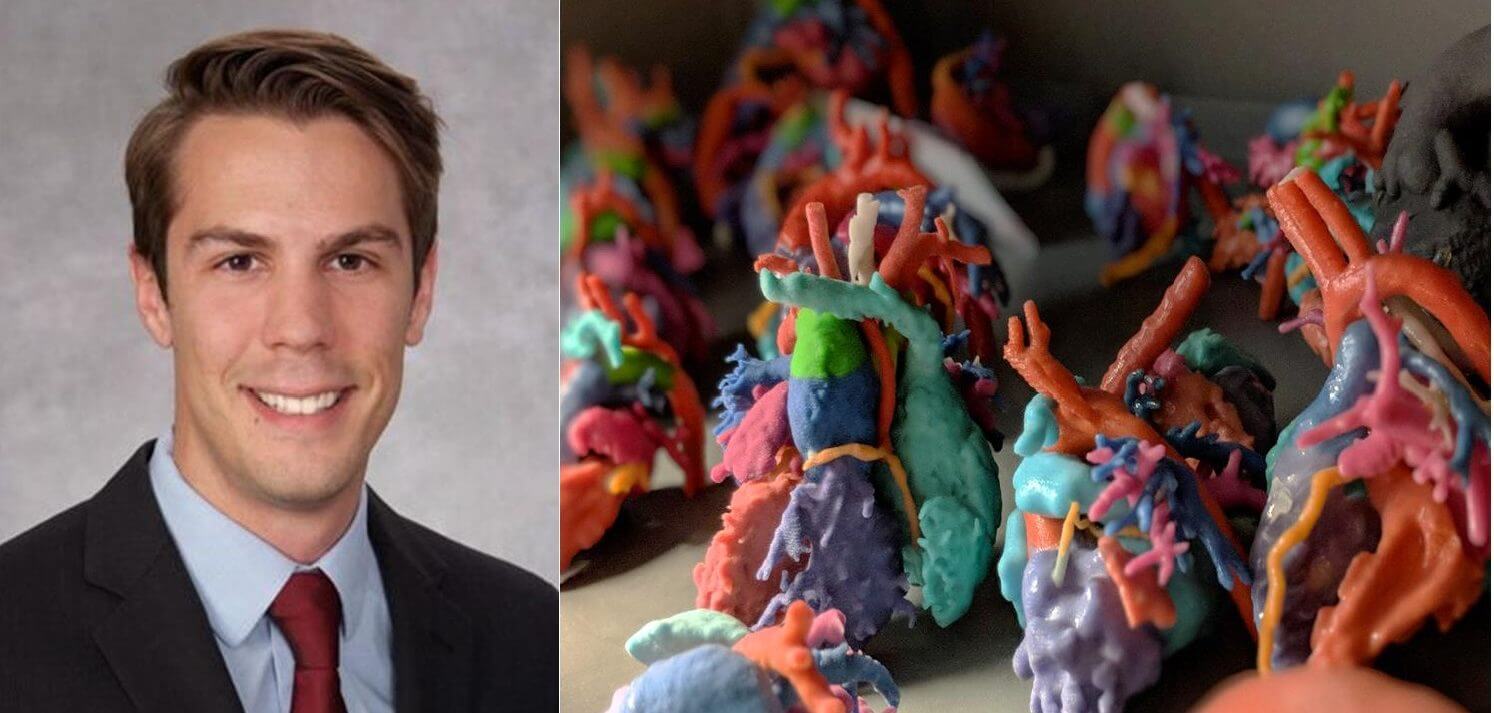
Rady Children’s Hospital in San Diego has established an Innovation lab that includes 3D printing and other emerging 3D technologies. Rady chose not to buy desktop 3D printers but the hospital opted for an HP 580 Color system. We interviewed Justin Ryan, director of Rady Children’s Hospital’s 3D Innovations Lab to find out more.
Why are hospitals now setting up 3D Printing labs?
More and more hospitals are recognizing the role of emerging additive manufacturing technologies (in conjunction with extended reality technologies such as virtual reality, mixed reality, and augmented reality). The technological potential afforded by 3D printing is straightforward – see the traditionally unseen and interact with anatomy without harming a patient. This added information – we perceive as a greater academic medical community – yields better-informed surgical and interventional procedures.
What parts are doctors asking for?
Every hospital is unique as to which departments embrace 3D printing. At our institution, we see strong use by orthopedics and cardiothoracic surgery. This utilization translates to the production of complex, congenital models such as scoliotic spines, dysplastic hips, and complex congenital heart disease models. Since bringing the technology in-house, we are seeing an increased use from our airway (specifically otolaryngology) and pediatric surgery teams. Essentially, whatever we can image we have the potential to print.
We are seeing that 3D printing is aiding in patients understanding consent and their particular pathology, are you?
We are absolutely seeing this technology used for consultation with families. In particular, that is why we embrace technologies that convey color information. When we are communicating with families we will point to a structure, use its actual name and also identify it by color. By using easier to digest anatomical names and color coding, we hope to better impart the critical information – after all, we want our families to have true informed consent. You cannot achieve that without families understanding these often dense medical terms associated with diagnoses and procedures.
What can a 3D printed model do for a surgical team?
Anatomical models provide surgeons and interventionalists an opportunity to review (and in some cases practice on) patient specific anatomy. For instance, they can review the unique angle and shape of a femur (thigh bone) and design a specific intervention to correct for malalignment. Another example is our cardiothoracic surgeon knows the shape, size, and location of a hole in the heart before ever stepping foot in the operating room. This hopefully translates to a faster, optimal surgery.

What is the path like from DICOM file to part?
The path from DICOM (medical imaging file) to part is institution specific, but typically follows a similar pathway. A technologist or operator (sometimes a radiologist or scientist) reviews the DICOMs in a software suite. The suite also enables them to segment (or define specific areas in an image set). These segmented structures are reconstructed into a 3D geometry. The operator may further refine the 3D dataset (e.g., cutting off features, coloring features, adding in guidelines). The resulting model is then saved and sent to 3D printers. DICOM (the organization behind the file format) is working on updating its specification to enable 3D files into its infrastructure. You can find more information at the Dicom Standard.
Why pick HP Jet Fusion 3D printing?
HP’s Jet Fusion 580 color 3D printing technology affords us some unique capabilities that altogether aren’t seen in a single printer. The PA12 nylon is a beautifully durable material. I can be confident that when I create a model and deliver it to the appropriate care team that the model will not break with typical handling. The coloring of anatomical models is also a fantastic ability – it helps promote communication between different hospital disciplines as well as facilitate the delivery of complex content knowledge to our patients and their families (who often don’t have a medical background). For example, it is much easier to have a visual aid when describing Tetralogy of Fallot with a patent ductus arteriosus and major aortopulmonary collateral arteries. It is a mouthful for even me to say let alone a non-medically educated parent who is going through stress of diagnosis and an upcoming surgery of their child.
Can 3D printed parts save costs?
As a greater academic medical community, we do have the perception that we are saving in the overall cost of care. We hypothesize that the models may yield lower complications or lower operative time. My colleague here Dr. Vidyadhar Upasani, a pediatric orthopedic surgeon at both UC San Diego and Rady Children’s Hospital, published a paper towards this goal of cost savings. We do need more clinical trials and larger studies to more definitively understand the impact of 3D printing in healthcare.
What other things (rather than surgical models) do you expect to be 3D printed at the hospital?
We are already exploring fabrication uses of 3D printing. We are collaborating with our simulation center, The Center for Innovative Learning, in designing educational simulators to better train our team. We are even exploring opportunities of device design and development. 3D printing is a whole new toolbox for any medical institution.
Do you foresee bioprinting happening in the hospital?
We are already seeing fantastic development in bioprinting and biocompatible printing from academic institutions. I think it will take several years to trickle its way down into hospitals, even then, a process like bioprinting may be relegated to technologically advanced third-party vendors (analogous to medical device manufacturers). As the process and technology get further refined, we may see this technology work its way direct into hospitals.
How about surgical guides?
Surgical guides are already being developed at point-of-care (inside hospitals). Different manufacturers already have sterilizable media for 3D printing. This translates to the possibility to create a surgical guide (or jig) to help guide surgical tools such as a saw or drill.
What is holding back 3D printing in hospitals?
Insurance reimbursement is the key for hospitals to truly embrace 3D printing and adjunct technologies. We as a community have come a long way. The RSNA Special Interest Group is one of the entities that is leading the effort in the development of insurance codes for reimbursement. In July of this year, the American Medical Association released 4 category 3 codes related to 3D printing. While these codes are not likely to yield high reimbursement (at least early on), it does enable the community to collect data on utilization that may yield a category 1 code at a later date. When our community receives proper reimbursement for 3D printing and adjunct technologies, we will see an increased development of 3D technology specific to our domain. This will hopefully translate to increased speed and integration into the medical framework.Other resources your readers may be interested in in the American College of Radiology, Society for Cardiac Magnetic Resonance, and the American Society of Mechanical Engineers.
Subscribe to Our Email Newsletter
Stay up-to-date on all the latest news from the 3D printing industry and receive information and offers from third party vendors.
Print Services
Upload your 3D Models and get them printed quickly and efficiently.










You May Also Like
Beyond Generative Design: Can AI-Driven 3D Printing Truly Deliver on Precision?
Artificial Intelligence (AI) has brought a new look to the hardware engineering domain. Using generative design algorithms, engineers put performance parameters and weight constraints together and the program generates complex,...
The Next Phase of EB-PBF Will Be Defined by Beam Control
The bar for metal additive manufacturing has moved. Early on, the question was often simple: Can the machine print the material and produce a dense part? That still matters, but...
The SLS Market, Game of Trucks: Part 2
With the release of the new HP 1200 and the Formlabs X1, we can see real competition from very different segments. From several million dollars to just $20,000, the laser...
Australia’s AMCRC Funds Titanium 3D Printing R&D
In terms of the global economy’s presently existing state, there is no realistic path to economic resilience that doesn’t start with critical minerals security. This is a problem for pretty...