Head & Neck Tumors: 3D Printing & Virtual Reality Aid in Surgical Planning


In the recently published ‘Combined application of virtual surgery and 3D printing technology in postoperative reconstruction of head and neck cancers,’ scientists from both the US and China collaborated on a study to integrate virtual and 3D printing applications into postoperative treatment of cancer.
The authors shared five cases taken on by the head and neck surgery department where reconstruction was performed. Reminding us that both the head and neck are ‘exceptionally complex,’ this is an area where organs, vessels, and nerves meet. When tumors grow in such an area, total resection is the only choice, and sometimes the surgery must be radical to ensure success.
While every surgery is important, removal of a tumor from the head or neck must be well-planned:
“In order to achieve complete resection and efficient and effective functional reconstruction, it is particularly important to develop a reasonable preoperative surgical plan and execute that plan in the operating room,” stated the researchers.
The use of typical 2D methods today like ultrasound, CT, or MRI may show the connection between a tumor and surrounding tissue, but further evaluation can be limited. As a result, surgeons are challenged to plan for surgeries comprehensively. Virtual surgery and augmented reality techniques, however, along with 3D printing and robotics, make it much easier for surgeons to create a personalized approach today for treatment, along with each step of a medical procedure, and post-operative measures.
Virtual reality simulates a digital 3D world, and for surgeries—especially that of a more complex area like the head and neck—it can actually be used in a capacity that ‘virtually’ replaces a human assistant, helps assess the course of action for the operating room, and acts as a surgical guide too.
“Applying VR technology to the head and neck can make complex structural relationships vivid and stereoscopic, making an abstract concept intuitive and clear, and bring great flexibility to the operative field. We recognize the importance of the application of CAD / CAM and VR technology in head and neck surgery,” stated the researchers.
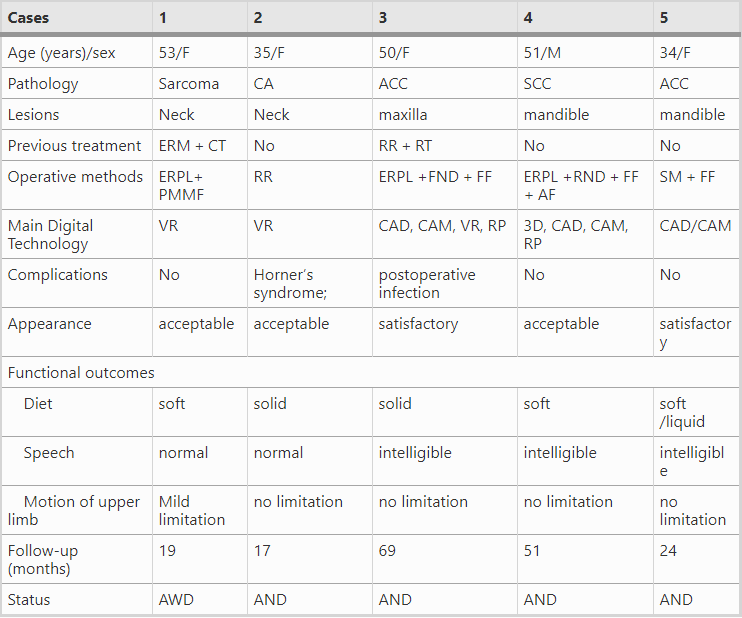
F female, M male, ACC adenoid cystic carcinoma, SCC squamous cell carcinoma, CA carotid aneurysm, CT chemotherapy, RT radiotherapy, FND functional neck dissection, RND radical neck dissection, RR radical resection, ERPL enlarged resection of primary lesions, MFF myocutaneous free flaps, FF fibula flap, LF Iliac bone flap, PMF pectoralis major flap, AF adjacent flaps, PMMF Pectoralis major muscle flap, ERM extensive radical mastectomy, SM segmental mandibulectomy, VR virtual reality, 3D three dimensional, CAD computer aided design, CAM computer aided manufacturing, RP rapid prototyping, AR augmented reality; Functional outcomes [diet (solid, soft, liquid, or nasogastric tube feeding), speech (normal, intelligible, slurred, or requirement for a tracheostomy), and range of motion of the upper limb (severe limitation, moderate limitation, mild limitation, no limitation)]; AWD alive with disease, AND alive with no disease
Case One – 53-year-old female with mass in her left neck, history of recurrent breast cancer, and multiple surgeries related to that. The biopsy showed that the mass in her left neck was malignant fibrous histiocytoma. Surgeons used VR to simulate the surgery, with the use of a 3D reconstructed model including:
- Color coding of important structures
- Blood vessels
- Nerves
- Bone
- Tumor
“Following use of the VR with multiple sessions, the patient underwent extended excision of left cervical and thoracic junction tumor with partial left clavicle resection, left subclavian vein repair, and pectoralis major myocutaneous flap repair under general anesthesia,” stated the researchers.
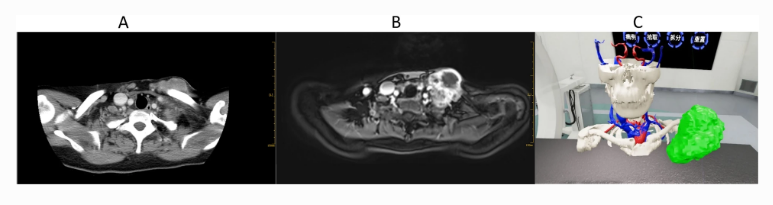
a CT shows the range of tumor invasion (cross section); b MRI shows the range of tumor invasion (cross section); c Surgical simulation which using gestures to pick up, rotate, zoom, model resolution, profile and other operations by VR technology
Case Two – 35-year-old female presented with 3 × 3 cm right neck mass, discovered during examination for a stroke. Surgeons used VR to create 3D printed models and simulate resection.
“After optimizing the preoperative planning, the patient underwent right carotid body tumor resection. VR allowed the surgeon to practice the gradual separation of the tumor at the carotid bifurcation,” stated the researchers.
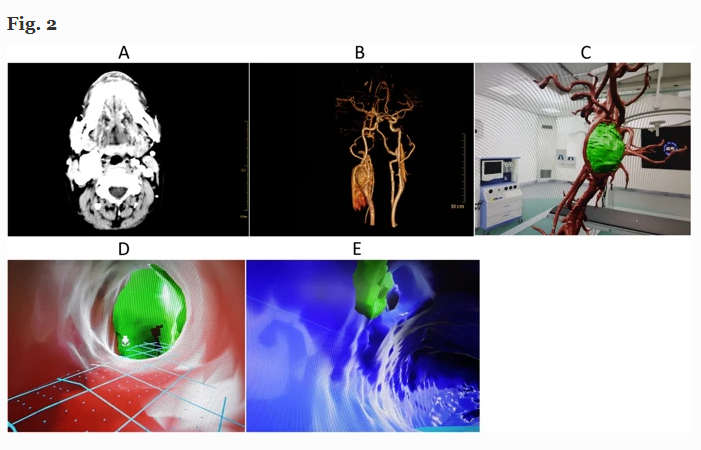
a CT shows the relationship between tumor and adjacent tissue; b CTA shows the relationship between tumor and blood vessel; c VR model after removal of the venous system; d Intravascular peep from the internal arteries of the carotid body tumor; e Intravascular peep from the vein of the carotid body tumor
Case Three – 50-year-old female with adenoid cystic carcinoma, presented with a 5.0 × 4.5 cm mass in her left cheek. A 3D model was created, and simulated reconstruction followed.
“The patient then underwent excision of the maxillary tumor, nasal septal resection, bilateral neck dissection, fibula myocutaneous flap repair, and abdominal free skin grafting. We use a 3D printed osteotomy plate after CAD design to precisely perform the appropriate osteotomies for resection of the tumor,” stated the researchers.

a CT transect showed that the lesion infiltrated into the left vestibule area, involving the nasal septum and the nasal floor; b Three-dimensional reconstruction of maxillofacial region, bone defect; c and lower extremity vessels by CAD technique after CT angiography; d Computer simulation for repair of maxillofacial region; e The position, length, arc of the fibula and the angle of the osteotomy of the fibula used by computer simulation and repair; f The effect of computer simulation after repair; g Three-dimensional printers’ rapid prototyping model; h The left maxillary tumor resection (resection including the left maxillary sinus wall, inferior wall, anterior wall, the section on the right side of the maxillary sinus and inferior wall, by simultaneous resection of nasal septum and nasal tumor infiltrating the bottom); i The skin flap was designed as the center of the skin before operation, and the skin of the left calf was cut into the perforator to dissect the perforating branch of the peroneal artery; j Vascularized free fibula myocutaneous flap was made by truncated fibula; k Repair effect of vascularized free fibula myocutaneous flap during operation
Case Four – a 51 year-old male was discovered to have a 2.5 × 3.5 cm left gingival squamous cell carcinoma. The left mandible was included, along with multiple ipsilateral lymph nodes. A 3D model was created, along with an osteotomy plate.
“A custom pre-bent plate was designed according to the computer simulation and the 3D model. We fixed the custom titanium plate at a predetermined position according to the simulation data and 3D model, and the oral defect was simultaneously repaired by the soft tissue component of the flap,” stated the researchers.
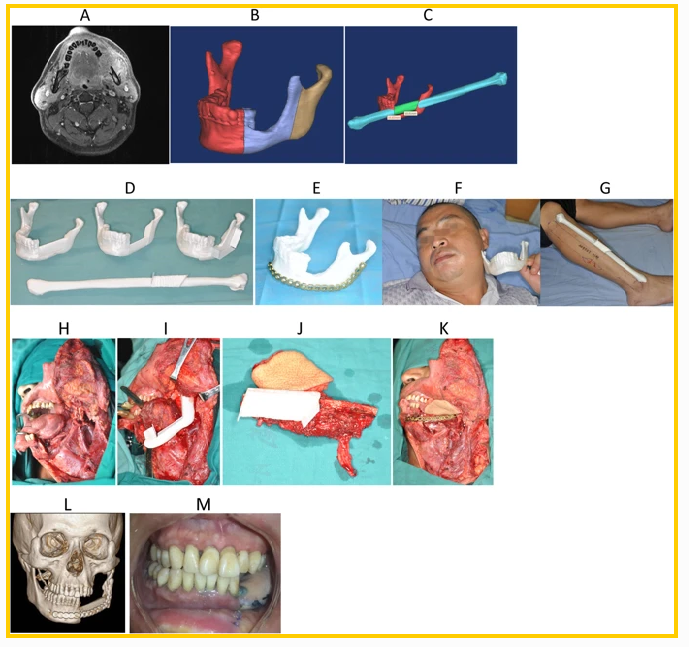
Preoperative performance and computer simulation of patients, model of rapid prototyping by 3D printer, one-stage repair of mandibular defect by CAD/CAM technique, and the follow-up of CAD/CAM assisted individualized repair of complex segmental defects in mandible. a The scope of invasion (transverse section); b The range of simulated surgical excision; c Osteotomy range and repair of simulated fibula flap; d Customize the osteotomy plate according to the model after the rapid prototyping, determine the interception range and location of the fibula; e Pre-bending of titanium plate according to the model after rapid prototyping; f The condition of mandible defect in patients with equal proportions; g The right fibula and osteotomy area of the equal proportions of the patients. h Expanded resection of tumor shows the area to be repaired; i The range of segmental resection of the mandible in the process of enlarged tumor resection is consistent with the preoperative simulation; j Preparation of free fibula flap according to the osteotomy plate model; k Repair of the defect area with free fibula flap and fixed with preformed titanium plate; l Three-dimensional reconstruction of CT scan in patients with postoperative lesions and repair and reconstruction; m The degree of occlusion was good and the function of the temporomandibular joint was normal
Case Five – a 34-year-old woman presented with a 5 cm left submucosal oral cavity lesion, also affecting several lymph nodes.
“A biopsy of the left mandibular mass showed fibrous lesions of bone which inclined to cementite fibroma,” stated the researchers.
“A three-dimensional solid model, osteotomy template of the lesion, and the iliac bone were developed through a 3D printer. Pre-bent titanium plates were prepared by the reconstructive model of rapid prototyping.”

a The CT in the maxillofacial region shown that the bone enlargement, destruction, and irregular mass of the mandible with a larger scope of approximately 5.5*3.1 cm; b Preparation of vascularized free iliac musculocutaneous flap; c Comparison of the prepared iliac bone flap with the 3D model; d Use of prefabricated titanium plates for fixing the disconnected mandible and the intercepted iliac bone; and e The second stage of dental implants; f The facial appearance and occlusion function after follow-up
“We conclude that computer-assisted surgery for personalized reconstruction of complex defects of the head and neck has role in clarifying tumor anatomy relationships, reconstructing complex osseous and soft tissue defects and defining vascular lesions such as aneurysms and vascular tumors,” stated the researchers, ultimately.
“This information leads to precise surgical treatment of head and neck cancer patients. However, its application in head and neck surgery is still limited. More systematic clinical results are needed to confirm the overall and reliable clinical value. Nonetheless, we believe that using computer-aided digital surgical technology to evaluate, simulate, formulate, and implement operative plans is an important trend in the future of head and neck surgery.”
What do you think of this news? Let us know your thoughts! Join the discussion of this and other 3D printing topics at 3DPrintBoard.com.
[Source / Images: ‘Combined application of virtual surgery and 3D printing technology in postoperative reconstruction of head and neck cancers’]Subscribe to Our Email Newsletter
Stay up-to-date on all the latest news from the 3D printing industry and receive information and offers from third party vendors.
Print Services
Upload your 3D Models and get them printed quickly and efficiently.










You May Also Like
The Next Phase of EB-PBF Will Be Defined by Beam Control
The bar for metal additive manufacturing has moved. Early on, the question was often simple: Can the machine print the material and produce a dense part? That still matters, but...
UAS Additive Strategies Shows How Fast Drone Manufacturing Is Changing
The recent UAS Additive Strategies online event, hosted by 3DPrint.com and Additive Manufacturing Research (AM Research), brought together leaders from across the additive manufacturing (AM) and drone industries to discuss...
The Drone Industry is Showing Where 3D Printing Delivers Real Value, AM Research Report Finds
The rapid rise of drones is creating one of the biggest opportunities for additive manufacturing (AM). Whether they’re used on battlefields, inspecting bridges or crops, or delivering supplies, drones need...
The Longevity Economy Needs a Factory
Longevity has become one of the biggest stories in healthcare. Every week seems to add a new announcement about an anti-aging therapy, an AI-powered drug discovery platform, or a startup...