There are more than 120 different types of brain tumors, many of which are cancerous, but the deadliest, and sadly most common, is the aggressive, fast-growing glioblastoma multiforme (GBM), a type of central nervous system tumor that forms on the brain’s supportive tissue. For several years now, researchers have been turning to 3D technologies to help better understand and treat this lethal disease, and the latest efforts are by a team of Tel Aviv University researchers, who used 3D bioprinting to fabricate an entire active, viable glioblastoma tumor.
The tumor, printed out of human glioblastoma tissues taken from actual patients at the Tel Aviv Sourasky Medical Center, includes a system of tubes, akin to blood vessels, that allow drugs and blood cells alike to flow through, in a simulation of an actual tumor. Led by Professor Ronit Ronit Satchi-Fainaro, Sackler Faculty of Medicine and Sagol School of Neuroscience, and PhD student Lena Neufeld, the results of the study were recently published in Science Advances.
“Glioblastoma is the most lethal cancer of the central nervous system, accounting for most brain malignancies. In a previous study, we identified a protein called P-Selectin, produced when glioblastoma cancer cells encounter microglia — cells of the brain’s immune system. We found that this protein is responsible for a failure in the microglia, causing them to support rather than attack the deadly cancer cells, helping the cancer spread,” explained Prof. Satchi-Fainaro, who is also the Director of the Cancer Biology Research Center, Head of the Cancer Research and Nanomedicine Laboratory, and Director of the Morris Kahn 3D-BioPrinting for Cancer Research Initiative, all at the university. “However, we identified the protein in tumors removed during surgery, but not in glioblastoma cells grown on 2D plastic petri dishes in our lab. The reason is that cancer, like all tissues, behaves very differently on a plastic surface than it does in the human body. Approximately 90% of all experimental drugs fail at the clinical stage because the success achieved in the lab is not reproduced in patients.”
Eilam Yeini, Noa Reisman, Yael Shtilerman, Dr. Dikla Ben-Shushan, Sabina Pozzi, Dr. Galia Tiram, Dr. Anat Eldar-Boock, and Dr. Shiran Farber—other researchers at Prof. Satchi-Fainaro’s laboratory—helped Neufeld develop this new technology. The bioprinted glioblastoma tumor model includes 3D cancer tissue that’s surrounded by an extracellular matrix, which uses functional blood vessels to communicate with its microenvironment and solve the problem about cancer behaving differently in the human body than it does on plastic.
“It’s not only the cancer cells. It’s also the cells of the microenvironment in the brain; the astrocytes, microglia and blood vessels connected to a microfluidic system — namely a system enabling us to deliver substances like blood cells and drugs to the tumor replica,” Prof. Satchi-Fainaro said. “Each model is printed in a bioreactor we have designed in the lab, using a hydrogel sampled and reproduced from the extracellular matrix taken from the patient, thereby simulating the tissue itself. The physical and mechanical properties of the brain are different from those of other organs, like the skin, breast, or bone. Breast tissue consists mostly of fat, bone tissue is mostly calcium; each tissue has its own properties, which affect the behavior of cancer cells and how they respond to medications. Growing all types of cancer on identical plastic surfaces is not an optimal simulation of the clinical setting.”

The team’s guess was that current cancer models are inadequate because they don’t have the necessary interactions between the tumor and stroma—the supportive tissue of an organ or tumor made up of blood vessels and connective tissues.
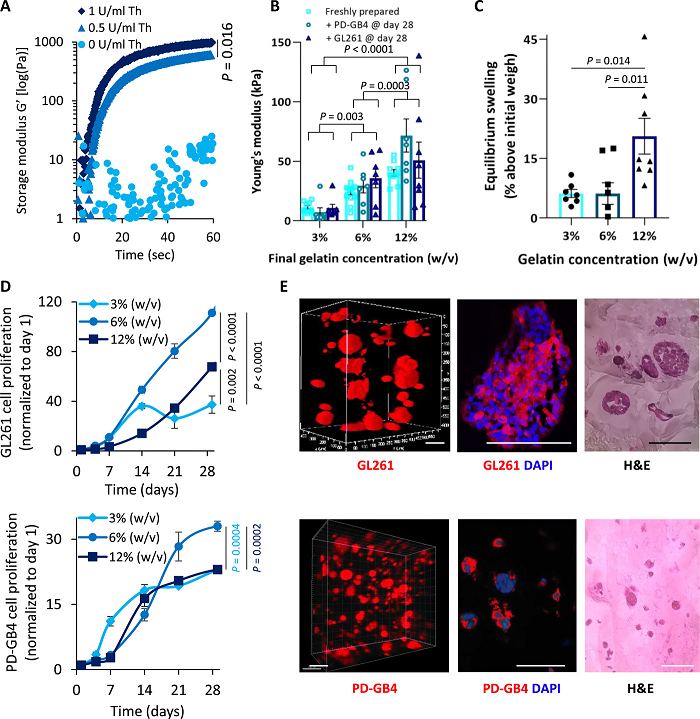
“Therefore, we recapitulated the tumor heterogenic microenvironment by creating fibrin glioblastoma bioink consisting of patient-derived glioblastoma cells, astrocytes, and microglia. In addition, perfusable blood vessels were created using a sacrificial bioink coated with brain pericytes and endothelial cells,” the researchers explained in their paper.
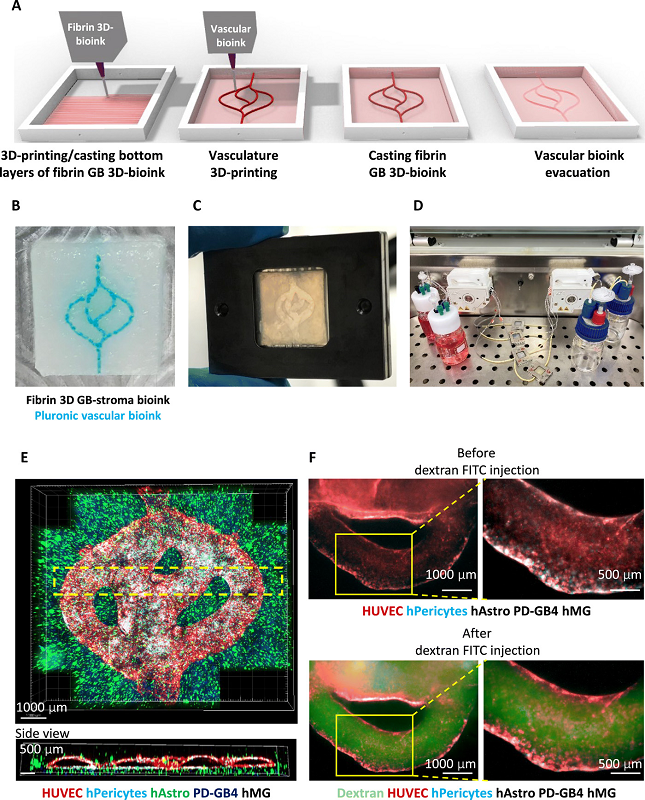
The team based its 3D engineered tissue constructs on a tumor bioink, made up of the natural polymers gelatin and fibrinogen, and a vascular bioink, composed of thermo-reversible biocompatible synthetic polymer Pluronic F127. As the researchers explained, due to its reversible gelation process, Pluronic F127 served as a sacrifical material “to fabricate embedded vasculature inside the 3D model and liquefied to create a 3D lumen vascular structure.”
They found that the 3D bioprinted model was more effective in terms of rapid, reproducible prediction of cancer treatment than petri dish cancer cells, which grow tumors and spread at the same rate. The researchers first tested a substance with the P-Selectin protein in glioblastoma cell cultures grown in 2D petri dishes, and found that there was no difference in cell division and migration between the control cells and the treated cells. But, by blocking this protein in animal models and their bioprinted model, they could successfully delay growth and invasion of glioblastoma.

“In addition, collaborating with the lab of Dr. Asaf Madi of the Department of Pathology at TAU’s Faculty of Medicine, we conducted genetic sequencing of the cancer cells grown in the 3D-bioprinted model, and compared them to both cancer cells grown on 2D plastic and cancer cells taken from patients. Thus, we demonstrated a much greater resemblance between the 3D-bioprinted tumors and patient-derived glioblastoma cells grown together with brain stromal cells in their natural environment. Through time, the cancer cells grown on plastic changed considerably, finally losing any resemblance to the cancer cells in the patient’s brain tumor sample,” Prof. Satchi-Fainaro said.
The major result of this experiment was proof that many potentially effective cancer drugs often don’t make it to human patients because they fail 2D model tests. The researchers believe that their new approach will enable new drug discovery and faster treatment predictions, and eventually expedite personalized medicine for cancer patients.

“If we take a sample from a patient’s tissue, together with its extracellular matrix, we can 3D-bioprint from this sample 100 tiny tumors and test many different drugs in various combinations to discover the optimal treatment for this specific tumor. Alternately, we can test numerous compounds on a 3D-bioprinted tumor and decide which is most promising for further development and investment as a potential drug,” concluded Prof. Satchi-Fainaro. “But perhaps the most exciting aspect is finding novel druggable target proteins and genes in cancer cells — a very difficult task when the tumor is inside the brain of a human patient or model animal. Our innovation gives us unprecedented access, with no time limits, to 3D tumors mimicking better the clinical scenario, enabling optimal investigation.”
(Source: ScienceDaily)