

Conventional simulators for intubation today are expensive and lack the anatomical accuracy needed. As a solution, South Korean researchers developed a new simulation model with 3D printing and silicone molding, releasing their findings in the recently published ‘Patient-specific and hyper-realistic phantom for an intubation simulator with a replaceable difficult airway of a toddler using 3D printing.’
Whether you have any experience in medicine at all or not, most likely you are somewhat aware of the intubation procedure and the fact that most patients have a strong desire to avoid the process. Far too many individuals are experiencing intubation today, due to complications from COVID-19. Training for medical students is also sometimes challenging, due to lack of accuracy in educational devices, as well as limited opportunities to actually intubate difficult cases; however, difficult tracheal intubation can cause serious respiratory issues or even death and improvements need to be made regarding education of medical professionals.
In developing the tracheal intubation simulator for this study and evaluating its true potential for training, the researchers focused on attending to details like jaw and cervical spine mobility, and tongue pressure in patients with Crouzon syndrome—a disorder causing premature fusion of the skull.
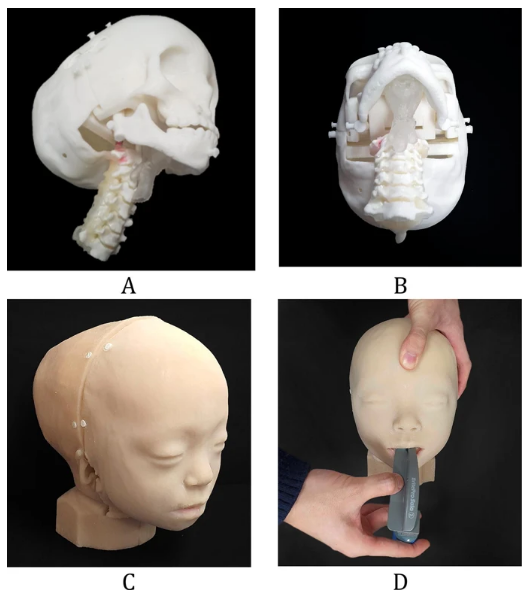
A patient-specific and hyper-realistic phantom for difficult tracheal intubation simulator. (A) Assembly of the inner parts, including the back of the skull, cranio-maxilla, mandible, cervical-spine, airway, and tongue in the isometric view. (B) At state, (A) bottom view. (C) Final phantom with front and rear skins. (D) Intubation with Macintosh blades in the phantom with mouth opening.
Employing three different 3D printers—a Form 2, an XFAB, and an Object J750—they created airway and tongue parts for the “phantom,” a simulator meant to appear similar to an individual with Crouzon syndrome.
“One of the most important factors of this phantom is the accuracy of mouth opening. The opening distance of the inter-incisor was set to 21, 32, and 47 mm. Two researchers measured these distances five times to analyze the accuracy of the opening distance of the mouth,” explained the researchers. “All the measurements were within the 95% limits of agreement.”
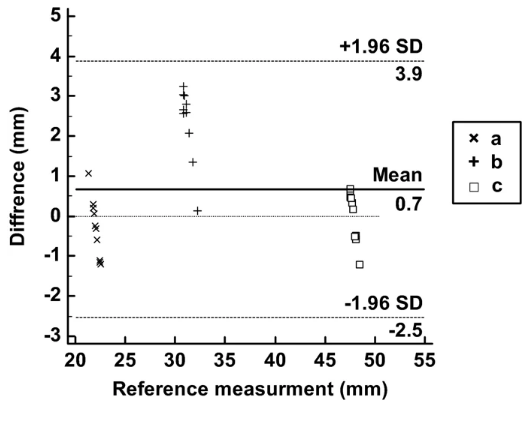
Bland–Altman plot to evaluate differences between the STL file and the phantom. (a) Measurements of STL and printed phantom at a 21 mm inter-incisor distance, (b) 32 mm inter-incisor distance, and (c) 47 mm inter-incisor distance.
In creating the samples, the researchers used CT data from images of an 18-month-old female toddler’s head. They specifically centered in on the following key parts:
- Skin
- Mandible
- Cranio-maxilla
- Skull
- Airway
- C-spine
- Tongue
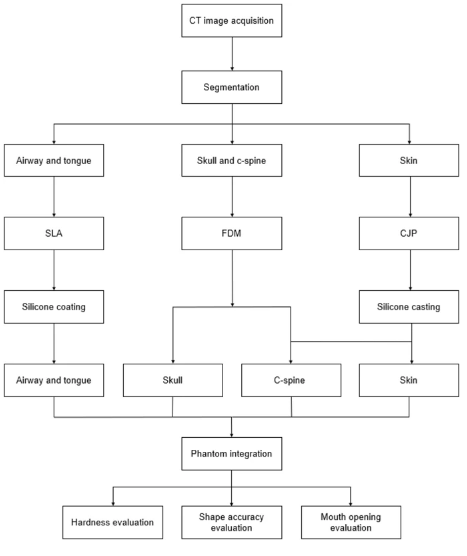
Overall procedure of manufacturing a difficult tracheal intubation simulator of a toddler. FDM fused deposition modeling, CJP color-jet printing, SLA stereolithography apparatus, C-spine cervical spine.
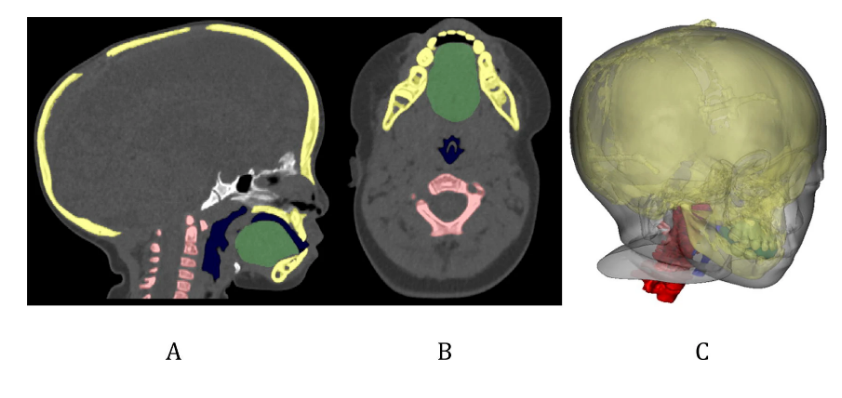
Visualization of segmentation with various anatomic regions for designing the difficult tracheal intubation phantom in CT images of an 18-month-old patient with Crouzon syndrome. (A) Sagittal view, (B) axial view, and (C) 3D visualization (cervical-spine, red; airway, dark blue; tongue, green; skull and mandible, yellow).
The airways and tongue were fabricated as one part, again, meant to be similar to a Crouzan syndrome patient. The tongue also had three joints, connected to a mandible, with both parts able to move together.
With 3D printed bone and soft tissue molded to imitate the human body, the researchers found the phantom to be successful—confirming the feasibility for use by those in training, and for use in practicing to intubate children as young as toddlers who are “developmentally compromised” or exhibit craniofacial anomalies.
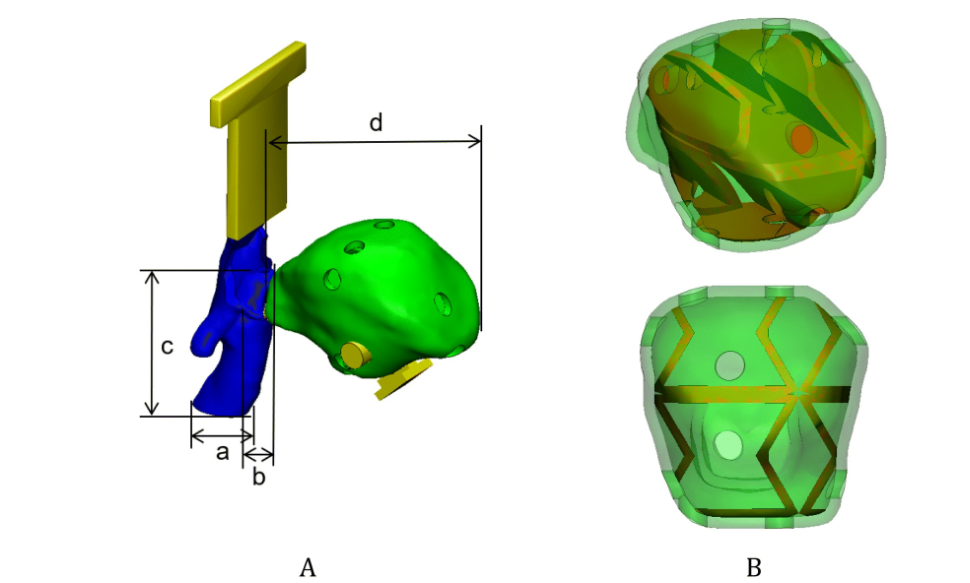
The airway and tongue were modeled based on CT images of a patient with Crouzon syndrome. (A) One part with the airway (blue) and tongue (green), and four measurements for evaluating fabrication accuracies, including (a) the inner diameter of the airway, (b) the width of the epiglottis, (c) the length between the epiglottis to the end of the airway, and (d) the length of the tongue (connectors to a mandible and cranio-maxilla; yellow). (B) inner structure (brown) and the outer hole of the tongue to mimic the tactile sensing to press the tongue with Macintosh blades and holes at the isometric (upper) and front (lower) views.
“Future work will focus on the generation of a variety of craniofacial anomaly models with the addition of an interchangeable model design that would bring this project one step closer to imitating reality, thereby enhancing the quality of training with models,” concluded the researchers. “We believe that the current 3D printing technology can narrow the gap between simulation-based medical education and authentic patient experience. For more realistic simulation, the patient-specific phantom was fabricated to mimic human tissue, with a realistic mouth opening and an accurate shape of the difficult airway, which has a great potential for the medical education and training field.”
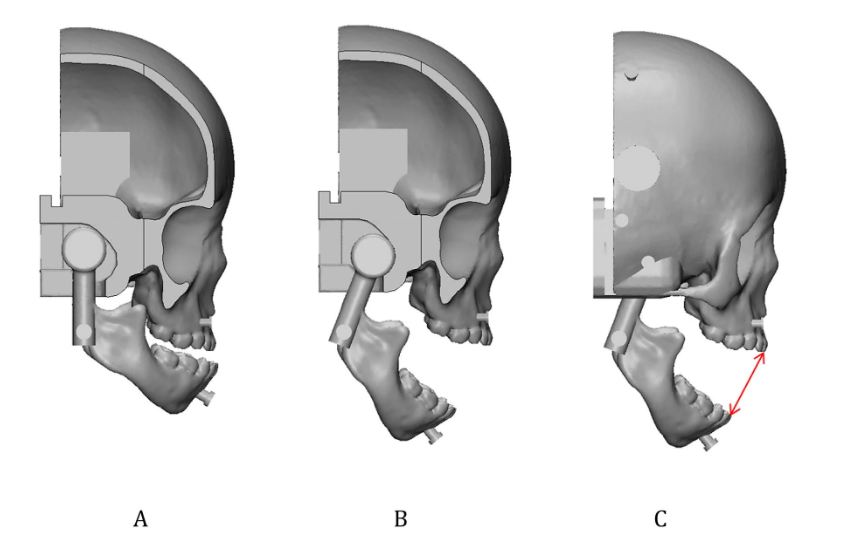
The overall design of the mouth movement. (A) The cranio-maxilla with a trailed socket inserted by a circular shaped condyle of the mandible at the closed mouth in the cutting at trailed socket. (B) The cranio-maxilla with the slid and rotated mandible at the open mouth in the cutting view. (C) At state (B), the length of the mouth opening in the inter-incisor distance in 3D visualisation was measured (red line).
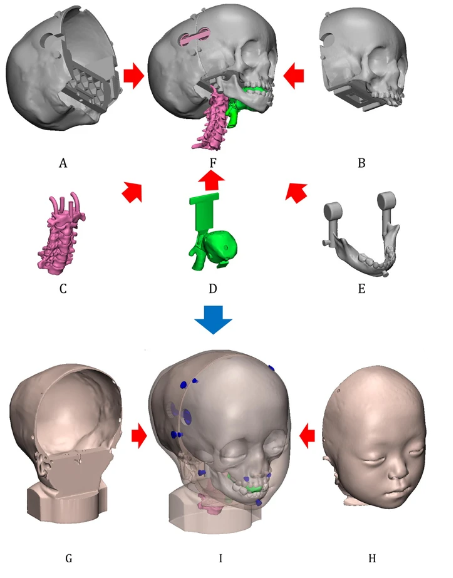
Assembly of difficult tracheal intubation phantom with various anatomic parts including (A) the back of the skull, (B) the cranio-maxilla, (C) the cervical spine, (D) the airway and tongue, (E) the mandible, and (F) the assembly of the inner structures including (A)–(E), excluding the skins. With skins including (G) rear and (H) front parts, all parts are assembled in (I) which integrates (F)–(H). The blue parts of (I) were used as connectors of the rear and front skins into the skull.
This new study follows current trends in the fabrication of simulators, solving cost issues, as well as offering a host of other benefits; for example, Singapore-based Creatz3D has designed and 3D printed life-sized medical mannequins that allow for medical training in swab collections for patients. International researchers have created a 3D printed phantom for greater ease in simulating procedures like administering epidurals, and experts at the 3D printing lab at Mayo Clinic’s Department of Neurosurgery—the B.R.A.I.N. (Biotechnology Research and Innovation Neuroscience) Laboratory have 3D printed a simulator to train medical students in spinal anatomy and pedicle screw placement.
[Source / Images: ‘Patient-specific and hyper-realistic phantom for an intubation simulator with a replaceable difficult airway of a toddler using 3D printing’]