

In the recently published ‘Trueness and precision of intraoral scanners in the maxillary dental arch: an in vivo analysis,’ authors Jonas Winkler and Nikolaos Gkantidis from the Department of Orthodontics and Dentofacial Orthopedics at the University of Bern in Switzerland are exploring ways to improve dental devices via 3D technology.
Intraoral 3D imaging is beginning to offer significant impacts within the dental field, especially because it allows for patients to receive oral cavity imprints that are without risk—as well as offering the following:
- Diagnosis
- Growth assessment
- Outcome evaluation
- Potential for use in 3D printing applications
“Digital dental models can overcome certain drawbacks associated with plaster models, such as patient discomfort and vulnerability. Being also advantageous in terms of cost, time, and space required, digital models will probably soon become the new standard in clinical practice,” explain the authors.
Intraoral scans are quickly becoming more useful in clinical settings; however, the researchers note that there is still a concerning amount of inaccuracy associated with such processes. Evaluating accuracy and precision is the goal of this study, and specifically in the fabrication of dental arches.

Box plots showing the trueness of the repeated intraoral scans with two different scanners in millimeters (n = 12, p = 0.176, Friedman test). The upper limit of the black line represents the maximum value, the lower limit the minimum value, the box the interquartile range, and the horizontal line the median value. Outliers are shown as black dots or stars, in more extreme cases. CS1, CS2, CS3: CS3600 repeated scans. TR1, TR2: TRIOS3 repeated scans. Artec: Artec Space Spider scan.
Eight male patients and four female patients participated, ranging in age from 27 to 52 years old. Three different scanners were used:
- CS 3600 (Carestream, Atlanta USA, Software CS Imaging Version 7.0.23.0.d2)
- TRIOS 3 (3Shape, Copenhagen, Denmark, Software Version 1.4.7.5)
- Artec Space Spider (Artec3D, Luxembourg, Software ArtecStudio 12 Professional Version 12.1.6.16)
“All scans were obtained by the first author who had more than two years of experience with regular clinical use of intraoral scanners,” explained the authors. “The same investigator performed all the steps of data generation following relevant training and under close supervision by the senior author.”
Irrelevant data like soft tissue were cropped out using Artec Studio 12 Professional software, and then the files were transferred for 3D printing. Final models were then superimposed in Viewbox 4, and the researchers used these settings:
- 100% estimated overlap of meshes
- Matching point to plane
- Exact nearest neighbor search
- 100%-point sampling
- Fifty iterations
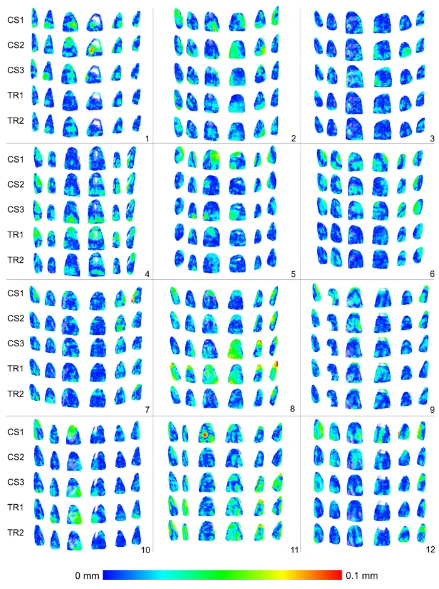
Colour maps showing the trueness assessment measured through the MAD of the CS3600 and TRIOS3 intraoral scanners from the gold standard scans, in the upper buccal front teeth area. Three scans obtained through CS3600 (CS1, CS2, CS3) and two scans through TRIOS3 (TR1, TR2) were assessed (n = 12 for each set of scans).
The research team noted ‘significant difference’ between the TRIOS 3 and the CS 3600, with the first demonstrating superior precision in two out of three cases.
“No specific imprecision patterns were observed in the respective color maps, since the errors were distributed equally between the different areas of the arch. However, in certain cases the imprecision was higher than in others. There was also significant variation within the arches, with local imprecisions reaching in several cases relatively high values,” explained the researchers.
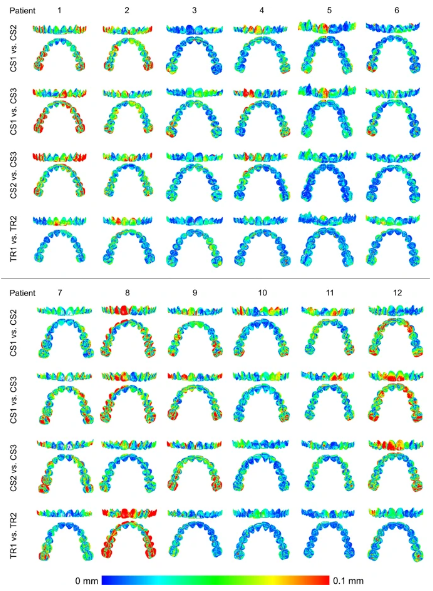
Colour maps showing the precision of the intraoral scanners. Three scans form CS3600 (CS1, CS2, CS3) and two scans from TRIOS3 (TR1, TR2) were assessed. The region for superimposition was the whole maxillary dental arch.
The Artec Spider was noted as ‘excellent’ in terms of scanning; in fact, it was chosen as a gold standard by the researchers.
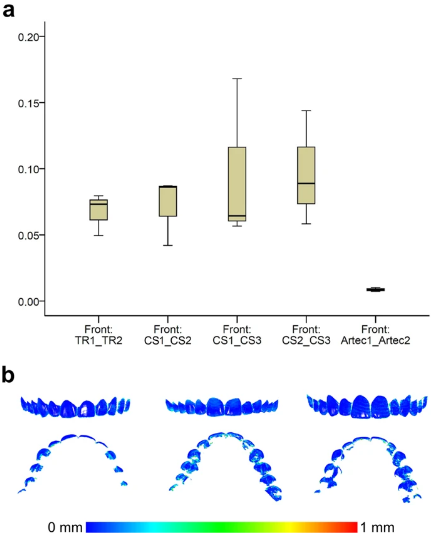
(a) Box plots showing the precision (millimeters) assessment of the gold standard scanner versus the intraoral scanners (n = 3), measured through the MAD of the whole dental arch area between repeated scans, when only the upper buccal front teeth area was used as superimposition reference. The upper limit of the black line represents the maximum value, the lower limit the minimum value, the box the interquartile range, and the horizontal line the median value. CS1, CS2, CS3: CS3600 repeated scans. TR1, TR2: TRIOS3 repeated scans. Artec1, Artec2: Artec Space Spider repeated scans. (b) Colour maps showing the absolute distances between corresponding points of surface models obtained through repeated scans with the Artec Spice Spider scanner.
“Both intraoral scanners showed comparable trueness in the upper buccal front region. Precision of the whole upper dental arch was also comparable when the repeated models were superimposed in the upper buccal front region. TRIOS 3 showed slightly higher precision (approximately 10 μm), when the whole model was used as superimposition reference, but it also showed the highest imprecision in a specific case,” concluded the researchers.
“However, in individual cases and in various, not spatially defined areas of the arch, higher imprecision was evident. In a small spatial scale, there is considerable variation in scanner performance between and within cases. Thus, the usage of intraoral scanners in highly demanding clinical applications, considering the whole arch, remains questionable.”
3D printing technology within the dental industry just continues to grow as some manufactures target mass production of products, improve fabrication of implants, continue to expand materials, and more.
What do you think of this news? Let us know your thoughts! Join the discussion of this and other 3D printing topics at 3DPrintBoard.com.
[Source / Images: ‘Trueness and precision of intraoral scanners in the maxillary dental arch: an in vivo analysis’]