Chinese researchers are using new technology to improve the total knee arthroplasty (TKA), outlining their findings in ‘Accuracy of a Novel 3D-Printed Patient-Specific Intramedullary Guide to Control Femoral Component Rotation in Total Knee Arthoplasty.’ As 3D printing continues to offer significant impacts within the medical field, the use of guides is becoming more common—and in this study, the authors focus specifically on the creation of a novel 3D‐printed patient‐specific intramedullary guide.
TKA is often used today to treat both pain and deformity in patients suffering from end‐stage knee osteoarthritis (OA). With well-known ‘good postoperative effects,’ TKA is the top choice for treatment in offering patients a better quality of life; however, as with many popular medications and treatments, there are numerous drawbacks—leaving over 20 percent of patients dissatisfied due to issues that include:
- Infection
- Aseptic loosening
- Joint instability
- Misalignment
- Periprosthetic fracture
- Patellar complications
“In the meantime, the accurate intramedullary guide of femur is the basis for ensuring the distal osteotomy of the femur,” explained the researchers. “Incorrect intramedullary guide will make it difficult to balance the inner and outer tension in the extension state of the knee, which will further lead to the imbalance of flexion and extension gap and eventually lead to the early failure of TKA.”
Ultimately, appropriate femoral resection and accurate component rotation are critical to a successful outcome. And while 3D printing has made major impacts in orthopedics, from offering industrial 3D printers to affordable methods for fabricating scaffolds, knee guides, hip guides, and more, in this study, the authors focus on combining 3D printing with patient‐specific instrumentation (PSI).
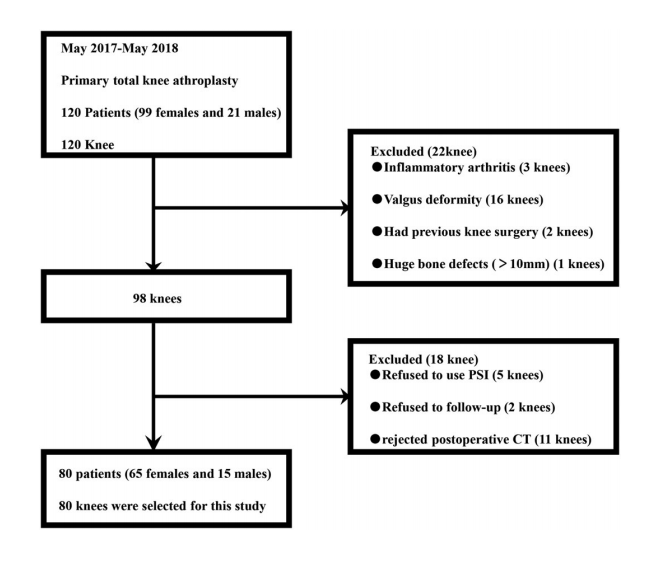
The study flow diagram
Performing a prospective randomized controlled trial (RCT) to show that 3DP‐designed PSI could outperform traditional TKA, the researchers evaluated postoperative radiological outcomes, accuracy in 3DP-designed PSI, and the actual feasibility for using the technology in the future. CT scans were converted to 3D printing files, printed out on an UP BOX, using bio-safe polylactic acid.
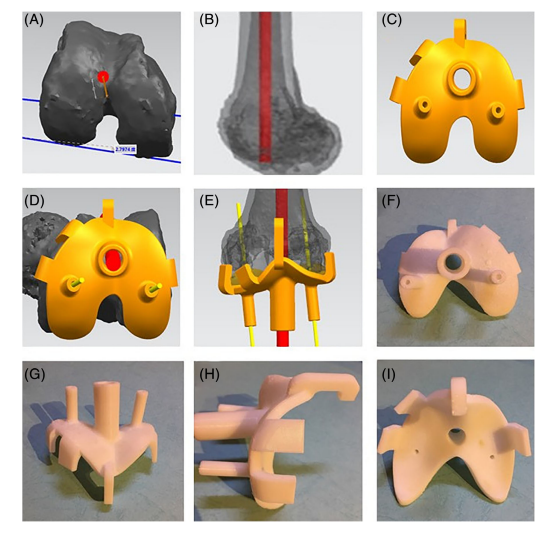
The process of designing PSI and the morphology of the PSI:(A, B) Finding the sTEA and the location of intramedullary guide; (C–E) The process of designing PSI; (F–I) The morphology of PSI in different perspectives.
Eighty patients (65 females and 15 males) participated in the study. They were placed into two groups (experimental, and control) randomly and were not aware of the use of PSI. One surgeon, with over ten years of experience in TKA, performed all the surgeries for the study, as each patient received the LEGION Total Knee System.
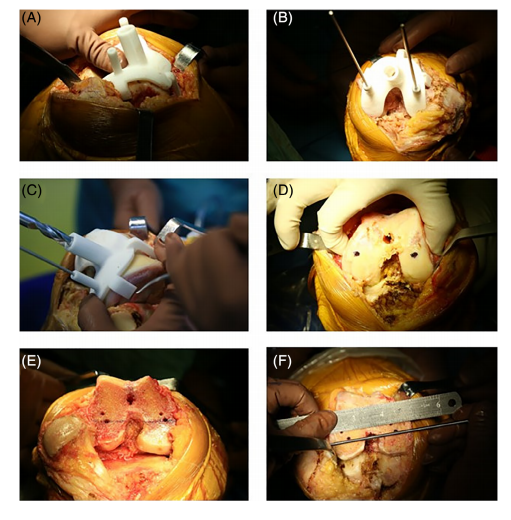
Steps of the TKA assisted by PSI technology representation: (A) PSI was placed on the distal femur surface; (B) PSI was fixed with Kirschner wire in order to mark the sTEA; (C) Drilling into the distal femur for intramedullary guide; (D) Palpating the medial and lateral epicondyles of the femur and observing the sTEA confirmed by the PSI; (E) Completing the distal femoral cuts; (F) Observing the relationship between the epicondylar axis determined by the femoral rotation guide and the sTEA confirmed by the PSI.
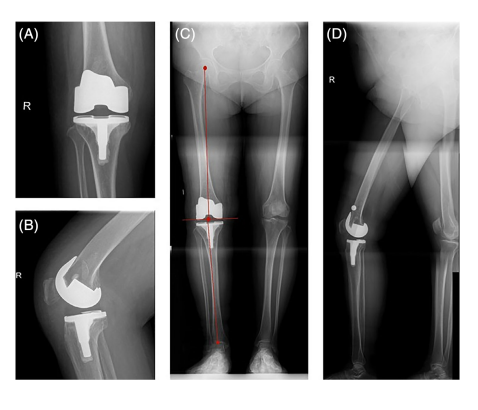
The postoperative radiographic examination of the knee and the full-length lower limb. HKA was determined in the coronal plane by measuring the angle (blue arrow) between a line connecting the center of the femoral head and the center of the knee (the red line on the side of the femur) and a line connecting the center of the knee to the center of the ankle (the red line on the side of the tibia) in radiographic images of full-length lower limb. HKA, hip-knee ankle angle.
After surgery, patients were followed for seven to twelve months, with all outcomes noted at the end.
PSI and conventional methods for the surgery were compared regarding the following:
- Clinical outcome
- American Knee Society knee score (AKS)
- Radiological outcomes
- Posterior condylar angle (PCA)
- Patella transverse axis‐femoral transepicondylar axis angle (PFA)
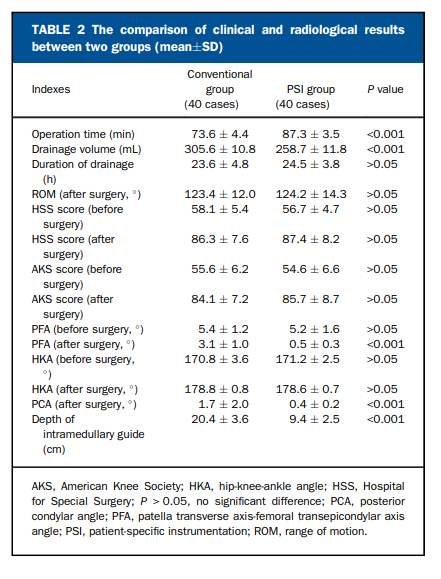
“PSI group had less postoperative drainage volume but longer operation time than the conventional group (P < 0.05). The AKS and HSS scores after surgery were improved compared with those before surgery in each group (P < 0.05). However, there was no significant difference in the duration of drainage and range of motion (ROM) after surgery between the two groups. For the radiological results, the HKA and PFA were improved after surgery in both groups (P < 0.05).The postoperative PFA and PCA of the PSI group were closer to 0°, which was better than that of the conventional group (P < 0.05). The depth of intramedullary guide in the PSI group was less than the conventional group (P < 0.05). But there was no significant difference in HKA before and after surgery between the two groups as well as the preoperative PFA,” concluded the researchers.
“Although TKA assisted by PSI spent more time during operation, it could assist in intramedullary guide and align femoral rotation more accurately.”
What do you think of this news? Let us know your thoughts! Join the discussion of this and other 3D printing topics at 3DPrintBoard.com.
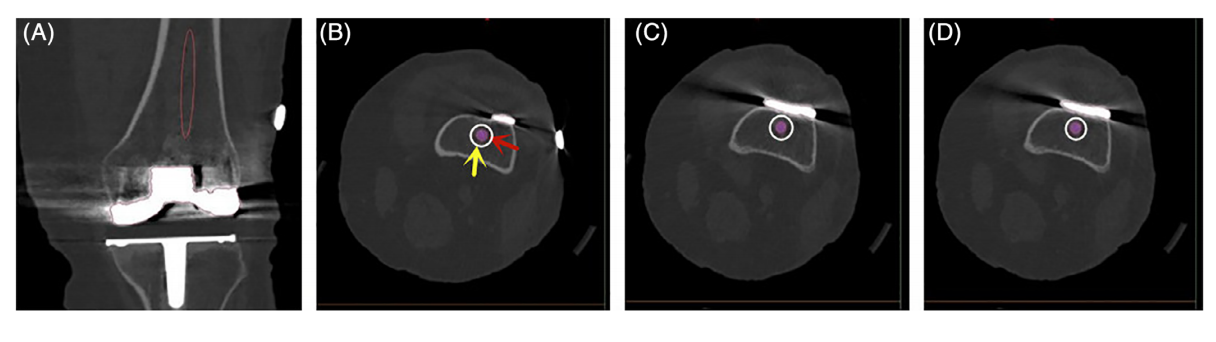
The location of preoperative designed and actual intramedullary guide: (A) The location of actual intramedullary guide (red circle); (B–D) The relationship between preoperative designed and actual intramedullary guide position on continuous CT level. The purple dot shown by the red arrow is the preoperative designed position, and the white circle area shown by the yellow arrow is the actual position.