
As is so often the case with 3D printing, the key is in customization—allowing for patient-specific treatment with a graft meant to apply to both horizontal and vertical augmentation of the atrophic alveolar ridge. With CT scans converted into data for creating completely customized grafts, treatment time is expected to be reduced and there is a greater chance for regeneration. This innovation accentuates the growing reliance of implants and prosthetics in resolving issues with appearance and chewing after tooth loss. Historically, dental implants can be challenging without the ability to customize extensively—and even with more patient-specific treatment, there are many obstacles that can come into play regarding successful implantation and regeneration.
Representative lateral views of virtual 3D models with small-defects.

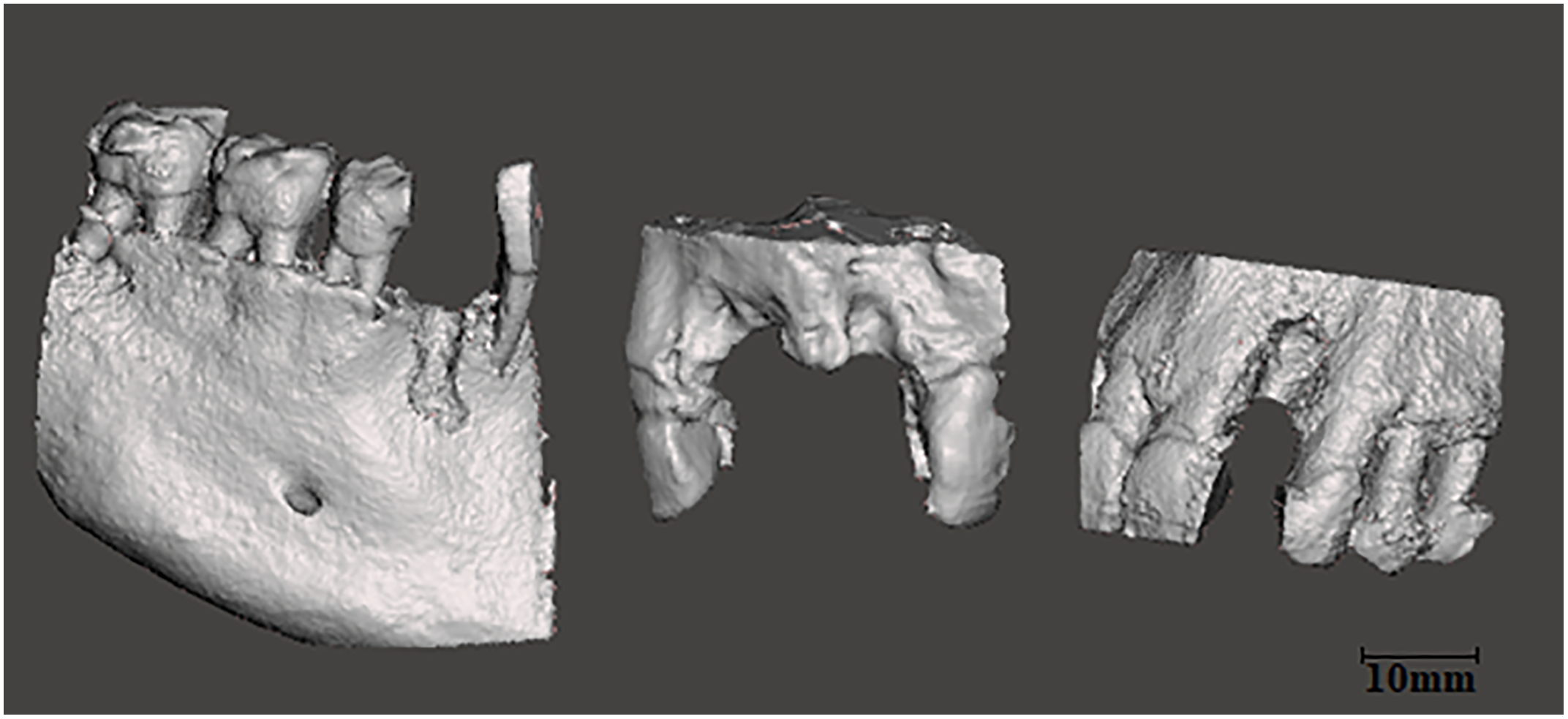
Lateral views of virtual 3D models with large-defects.

(A) Frontal view of a CAD mandibular model. (B) Lateroinferior view of a CAD large mandibular graft. (C) Frontal view of the graft fitted on the recipient site of the mandible. (D) Frontal CBCT view of the fitted graft.
The amount of bone volume left plays a large role in success, along with the types of defects involved—whether they are due to gum disease, cysts or tumors, teeth being pulled, or trauma to the mouth or jaw. There is also a range of different categories for defects, with the worst scenario being both horizontal and vertical defects occurring simultaneously.
“In situations of major changes in both vertical and horizontal bone dimensions, the placement of dental implants without an augmentation procedure could be very complicated or even impossible,” state the researchers.
Guided bone regeneration is usually a long process, and surgeons rely on a mixture of both biological and mechanical properties. Autogenous bone blocks are often used in surgeries, with grafts secured on the ridge or in between areas of pedicled and internal cancellous bone. The researchers state that success often relies on integration of the blocks as well as how well graft edges are smoothed, their stability, and their shape:
“The ideal biomaterial should be customized to fit easily on or into the corresponding bone defect and to allow proper fixation,” state the researchers. “The optimal shape of the graft may come with multiple advantages in terms of: (A) Faster surgical procedures, (B) Better healing of the grafted site, (C) Reduced risk of peri- and post-operative complications, (D) Higher success rates of the bone augmentation procedure and (E) Higher patient satisfaction.”
Shaping of bone grafts can be complex and requires an experienced hand. Without the proper expertise, healing may be unsuccessful.
“For this reason, there is a clinical need for customized biomaterials shaped to fit the patient’s bone defects,” said the authors.
With the options available through CAD design, bone defects can be scrutinized more closely, and customized, accurate grafts can be created before surgery. The entire process is more streamlined, surgical procedures are faster, and the patient has a better experience all around.
Six patients from the clinic of Oral Implantology and Prosthetic Dentistry at the Academic Centre for Dentistry Amsterdam (ACTA) were involved in the study, with the researchers evaluating cone beam computed tomography (CBCT) datasets from each, to be treated with implants and augmentation with bone blocks. Patients all presented as:
- Partially dentate
- Combined vertical and horizontal defect of the maxilla (three patients)
- Combined vertical and horizontal defect of the mandible (three patients)
3D reconstruction was completed for each patient’s jaw, with data imported into Meshmixer for design:
“The atrophic bone areas were defined separately for each jaw model in the edentulous part of the jaw. Because of the bone loss it is not possible to place an implant on this part of the jaw,” stated the researchers. “The customized grafts could be manually drawn directly on the surface of the 3D projects by fabricating the original shape of the jaw.”
The void interface set at 0mm between model and graft. The models (n = 6) were evenly divided in two groups, according to the number of missing teeth whether categorized as small defect or large defect. 3D printing was completed on a Form2 3D printer, with the following settings:
“Print resolution was set at 100 microns. To standardize the procedure, every graft and model was printed separately in the center of the build platform with a 135-degree build angle. The print supports were set on the external outline to prevent them interrupting the critical internal area. After printing, the objects were washed twice in two separate 90 percent isopropyl alcohol baths (10 min each) and were postcured for 30 minutes at 45° using a 405nm light box, according to the manufacturer’s protocol.”
The grafts were assessed in vitro, with each one serving as a match for the defect. The researchers state that large-defect grafts did not require any further refining, while small-defect grafts matched after some effort in manually smoothing undercuts. Results of the study were a success, supporting the idea that it is possible to both design and 3D print grafts for alveolar bone augmentation. The researchers state, however, that workflow for this process needs validation in a clinical setting; further, ‘proper vascularization’ must be ensured.
Materials must also be further analyzed for the following:
- Biocompatibility
- Osteoconductivity
- Surface porosity
- Surface chemistry
- Tissue bonding
- Material strength
- Degradation rate
“The marginal fit of the grafts was better than the internal fit, while the average void dimensions seemed to be correlated to the defect type of the graft. Further in vitro studies with 3D printable bone substitutes are needed for the validation of this digital workflow for alveolar bone augmentation,” concluded the researchers.
While 3D printing has permeated so many complex industrial applications, it may seem surprising to many that it could improve issues having to do with your teeth, mouth, and jaw, also—but just as the technology is becoming more affordable and accessible to others around the world, now so are better dental products and processes, including items like orthodontic aligners, removable partial dentures, and high-performance dental 3D printers available to labs.
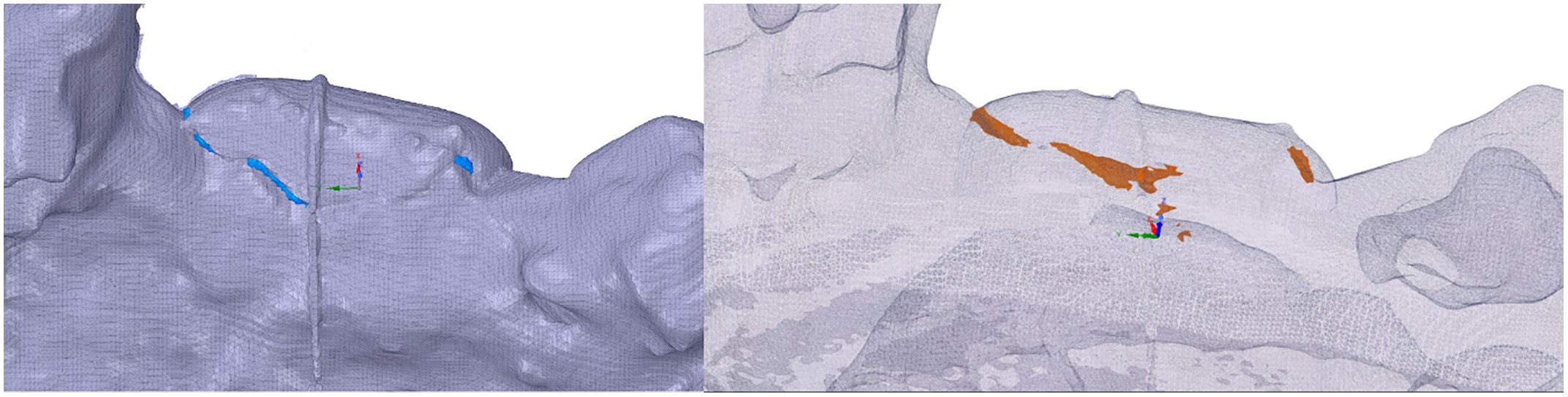
Blue and orange colored volume of the void between model and graft.